Tuberculosis summary
•
3 likes•1,647 views

Tuberculosis is caused by infection with Mycobacterium tuberculosis. It typically affects the lungs but can spread to other organs. Primary TB occurs after initial exposure and may result in an asymptomatic Ghon focus or spread to lymph nodes and other sites. Secondary TB occurs from reactivation of a dormant lesion, usually in the apices of the lungs. Diagnosis involves testing sputum, blood, or other fluids for acid-fast bacilli on smear or culture. Chest x-ray may show consolidations, cavities or fibrosis. Treatment involves a multi-drug regimen over 6-9 months to prevent resistance, with monitoring of side effects like hepatitis and optic neuritis. Contact tracing and screening of household members is

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Tuberculosis summary
Similar to Tuberculosis summary (20)
More from Dr. Rubz
More from Dr. Rubz (18)
Tuberculosis summary
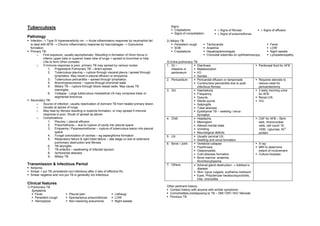
- 1. Tuberculosis Signs Crepitations ± Signs of fibrosis ± Signs of effusion Signs of consolidation ± Signs of pneumothorax Pathology Infection → Type IV hypersensitivity rxn → Acute inflammatory response by neutrophils fail 2) Miliary TB to deal with MTB → Chronic inflammatory response by macrophages → Granuloma Persistent cough Tachycardia Fever formation. SOB Anaemia LOW Primary TB: Crepitations Hepatosplenomegaly Night sweats o First exposure, usually asymptomatic. Resulting in formation of Ghon focus in Choroidal tubercles on ophthalmoscopy Lympadenopathy inferior upper lobe or superior lower lobe of lungs + spread to bronchial or hilar LNs to form Ghon complex. 3) Extra-pulmonary TB o If immune response is poor, primary TB may spread by various routes: 1. GI – Diarrhoea Peritoneal fluid for AFB 1. Progressive Pulmonary TB – direct spread. intestine or Malabsorption 2. Tuberculous pleurisy – rupture through visceral pleura / spread through peritoneum I/O lymphatics. May result in pleural effusion or empyema. Ascites 3. Tuberculous pericarditis – spread through lymphatics 2. Pericardium Pericardial effusion or tamponade Requires steroids to 4. Bronchopneumonia – rupture through bronchial walls Constructive pericarditis due to post- reduce need for 5. Miliary TB – rupture through blood vessel walls. May cause TB infectious fibrosis pericardiectomy meningitis. 3. GU Haematuria 3 early morning urine 6. Collapse - Large tuberculous mediastinal LN may compress lobar or Frequency for AFB segmental bronchus. Dysuria Renal U/S Secondary TB: Sterile pyuria IVU o Source of infection: usually reactivation of dormant TB from healed primary lesion. Salpingitis o Usually at apices of lungs Tubal abscess o May heal by fibrosis resulting in tubercle formation, or may spread if immune Epididymal TB – swelling / sinus response is poor. Route of spread as above. formation o Complications: 4. CNS Headache CSF for AFB – fibrin 1. Pleurisy ± pleural effusion Meningism web, mononuclear 2. Pneumothorax – due to rupture of cavity into pleural space Altered mental state cells, cell count 10- 3. Empyema / Pyopneomothorax – rupture of tuberculous lesion into pleural Vomiting 1000, ↓glucose, N/↑ space Neurological deficits protein 4. Fungal colonization of cavities – eg aspergilloma formation 5. LN Usually cervical LN. 5. Respiratory failure & right heart failure – late stage cx due to extensive Swelling and sinus formation pulmonary destruction and fibrosis 6. Bone / Joint Vertebral collapse X-ray 6. TB laryngitis Pyarthrosis MRI to determine 7. TB enteritis – swallowing of infected sputum. Osteomyelitis extent of involvement 8. Ischiorectal abscess Cold abscess formation Culture biopsies 9. Miliary TB Bone marrow: anaemia, thrombocytopenia Transmission & Infectious Period 7. Others Adrenal gland destruction → Addison’s Airborne. disease Smear + pul TB considered non-infectious after 2 wks of effective Rx Skin: lupus vulgaris, erythema nodosum Smear negative and non-pul TB is generally not infectious. Eyes: Phlyctenular keratoconjunctivitis, iritis, choroiditis Clinical features 1) Pulmonary TB Other pertinent history: Symptoms Contact history with anyone with similar symptoms Fever Pleural pain Lethargy Comorbidities predisposing to TB – DM/ CRF/ HIV/ Steroids Persistent cough Spontaneous pneumothorax LOW Previous TB Hemoptysis Non-resolving pneumonia Night sweats
- 2. Investigations Continuation phase Rifampicin & As above Microbiology Samples: sputum, induced sputum (using nebuliser), laryngeal swab and (4 mths on 2 drugs Isoniazid direct smear, NG aspirate (pump in saline and withdraw in the morning), Ethambutol 15mg/kg/day PO For resistant TB BAL, pleural fluid, pleura, urine, pus, ascites, CSF ZN or auramine stain Common & Important ADRs o + in 30% (up to 70%) Rifampicin Hepatitis Stop if bilirubin rises o Indicates high bacterial population and infectiousness. Cholestasis o Not specific for MTB. May be other mycobacterial spp. Orange discoloration of urine & tears C/S Severe thrombocytopenia o + in 66% Visual changes o Specific for MTB Liver enzyme inducer Caution in concurrent use with o Average 12-14 days for + result to return, another 1-2wks for OCP, warfarin, steroids, OHGA, sensitivity results phenytoin & digoxin. o Culture usually kept for up to 8 wks if negative Isoniazid Hepatitis Radiology CXR: Neuropathy, encephalopathy Give pyridoxine (Vit B6) to prevent o consolidation, cavitations, fibrosis, calcification / tuberculoma, collapse Pyridoxine deficit o Post TB bronchiectasis (usu upper lobes) Agranulocytosis o reticular-nodular opacities in miliary TB Pyrazinamide Hepatitis Mantoux Tests skin sensitivity to tuberculoprotein. + = sensitivity, NOT active infxn Arthralgia, gout Contraindicated in gout test (only 20% of infected individuals devt active infxn). May be + during Ethambutol Optic neuritis Test color vision before initiating Rx dormant OR active infection. Gout Inject 0.1ml of PPD intradermally Streptomycin Vestibular disturbance / ototoxicity Test for hearing before initiating Rx Read at 2-4 days: + if induration >10mm (locally 15mm), − if <5mm Nephrotoxicity False −: in sarcoidosis, malnutrition, Hodgkin’s dz, immunosuppression and overwhelming active TB Second line drugs: False +: atypical mycobacterial infections o Aminosalicylic acid Main use for contact tracing, to treat for latent TB infection o Cycloserine Serology o Ethionamide γ-interferon Eg Quantiferron, Elispot o Ofloxacin / Ciprofloxacin assays More sensitive c.f Mantoux test, but expensive. Not routinely done yet. Meningeal, ureteric and pericardial disease: consider adding steroids to reduce risks of Cx from scarring Monitoring of Rx efficacy – AFB smear & culture @ 2mths of Rx and after completing Rx, Management plus CXR after completing Rx. 1) Isolation For infectious pulmonary TB PTs. 3) Consider HIV testing Stop isolation only after >2 sputum cultures are AFB negative esp if high-risk group, or young (who don’t usually get TB. ?HIV) 2) Chemotherapy 4) Contact tracing & notification Check liver and renal functions, as well as color vision due to ethambutol ocular toxicity. Household contacts of sputum-smear positive PTs Give Pyridoxine throughout treatment to prevent isoniazid induced neuropathy 2/3-step contact tracing Directly Observed Therapy (DOT) to ensure compliance – daily Rx at TB control unit (CDC) o week 0 – do Mantoux, read at day 2-4 and polyclinics. Alternative: Intermittent DOT (3x/week). 97% cure rate ♦ if >15mm, means seroconvert – give prophylaxis ♦ if <15mm, repeat Mantoux Short-course regimen o week 2 – do Mantoux Initial phase (8 wks *Rifampicin 600-900mg PO 3X/wk ♦ if increase cf week 0’s test by >10mm, means that first /2mths on 3-4 drugs) *Isoniazid 15mg/kg PO 3X/wk Mantoux reactivated previously exposed immune system, now *Pyrazinamide 2.5g PO 3X/wk pt is displaying competent immune response – don’t need Monitor LFTs wkly Ethambutol 30mg/kg PO 3X/wk Add ethambutol or prophylaxis Streptomycin 0.75-1g/day IM streptomycin if ♦ if <10mm, do third Mantoux resistance is suspected.
- 3. o week 12 – do Mantoux ♦ if increase >10mm cf week 0, means pt has seroconverted, pt has LTBI, give prophylaxis ♦ if increase <10mm, no need prophylaxis 5) Chemoprophylaxis Consider for: o Severely immunosuppressed PTs (eg HIV +) o Unvaccinated contacts with recent MT + Isoniazid 300mg/day PO for 9 mth/ rifampicin 4 months if Mantoux positive as described 6) BCG vaccination at birth. Only protects against childhood miliary and CNS TB. Repeat vaccination in adolescence not found to affect outcome / risk of TB, and is no longer indicated. 7) Rx of Latent TB Infection Preventive ChemoRx Isoniazid (6mths locally, 9mths in USA) – effective in eradicating latent TB in 70%. Resistance to isoniazid not known to occur in the remainding 30% despite monotherapy. Digitally signed by DR WANA HLA SHWE DN: cn=DR WANA HLA SHWE, c=MY, o=UCSI University, School of Medicine, KT-Campus, Terengganu, ou=Internal Medicine Group, email=wunna.hlashwe@gmail.com Reason: This document is for UCSI year 4 students. Date: 2009.02.24 14:06:33 +08'00'