Downloaded 212 times

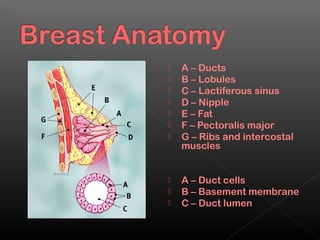
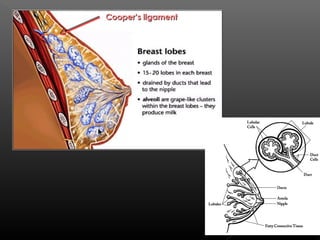
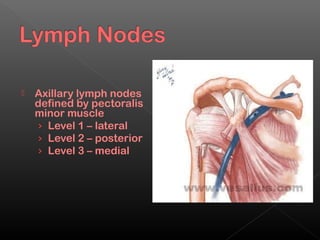
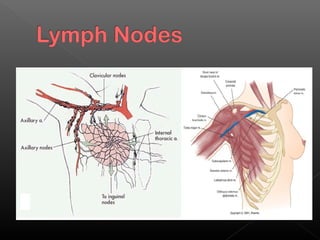


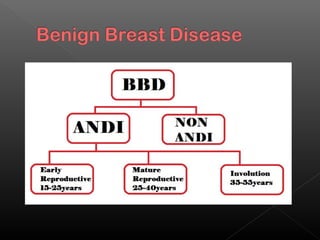


The document describes the anatomy and physiology of the breast as well as common breast conditions. It discusses the structure of the breast including lobes, lobules, ducts, and surrounding tissues. It then covers common benign and malignant breast diseases like fibroadenomas, cysts, mastitis, and ductal carcinoma in situ. The document concludes with descriptions of clinical exam findings, imaging tests, biopsy procedures, and management of various breast abnormalities.































































































