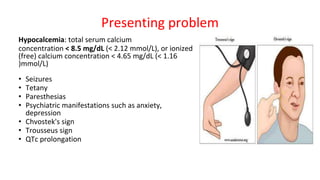
This document provides information about the parathyroid gland, including its anatomy, physiology, diseases, and presenting problems. It discusses the following key points:
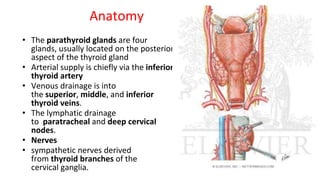
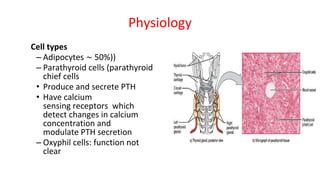
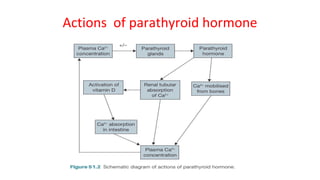
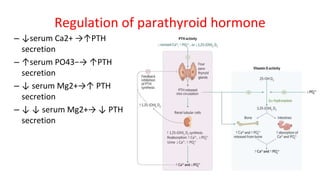
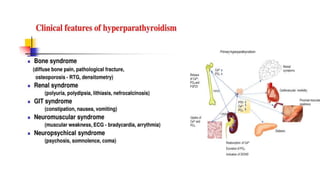
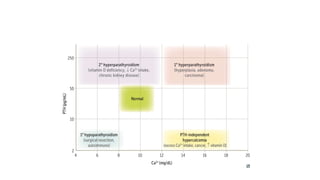
- The parathyroid glands regulate calcium levels in the blood through secretion of parathyroid hormone (PTH). High calcium levels decrease PTH secretion while low calcium increases it.
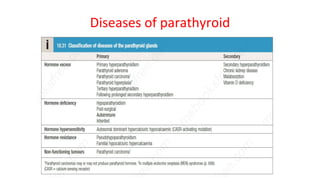
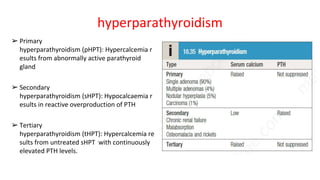
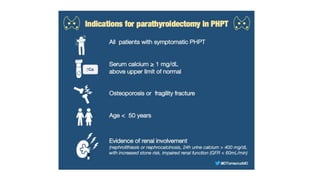
- Primary diseases include primary hyperparathyroidism from overactive parathyroid glands and hypoparathyroidism from underactive glands.
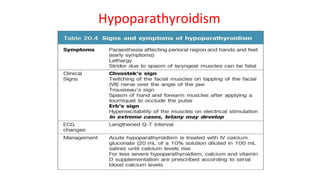
- Hyperparathyroidism causes hypercalcemia and is usually treated by surgically removing the overactive gland(s). Hypoparathyroidism causes hypocalcemia and is treated with calcium and vitamin
























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















