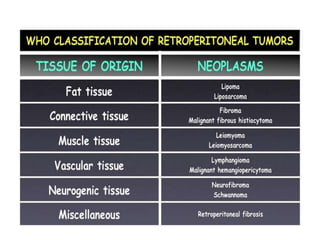
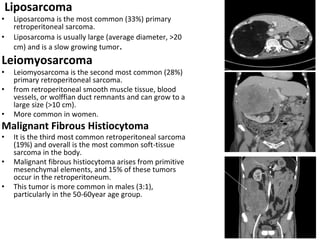
The document discusses retroperitoneal masses, which can be classified as solid or cystic, neoplastic or non-neoplastic. Common solid neoplastic masses include liposarcoma, leiomyosarcoma, and malignant fibrous histiocytoma. Neurogenic tumors and lymphomas also occur. Presentation is usually nonspecific symptoms or a large abdominal mass. Investigation involves blood tests, imaging like CT, and biopsy. Wide surgical resection is the standard treatment when possible.