Downloaded 404 times
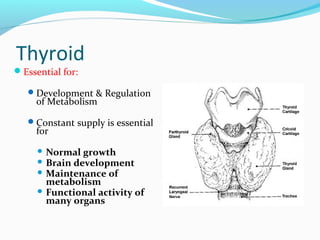
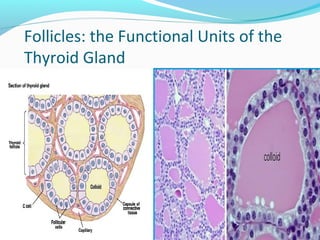






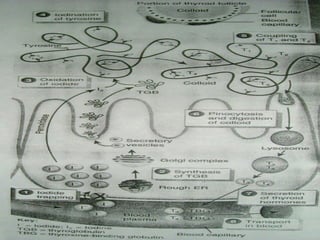
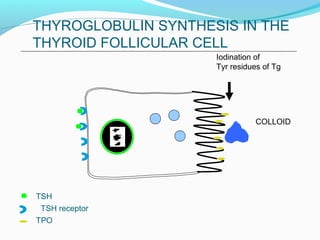
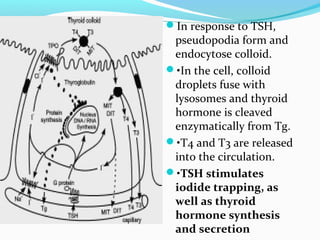
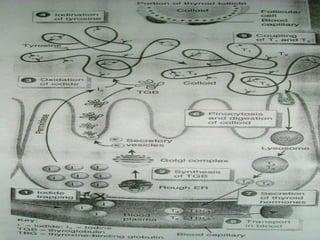







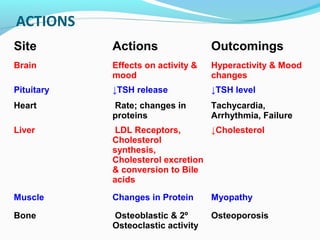
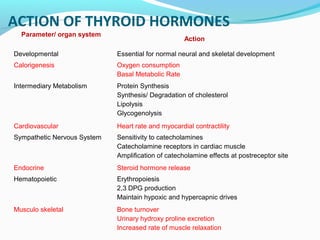


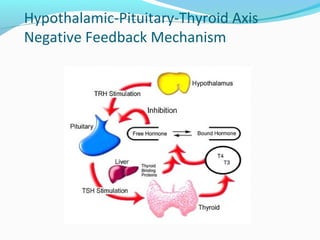
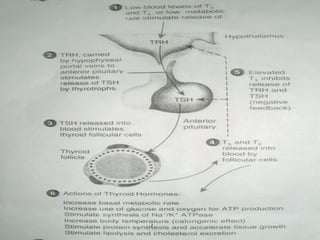

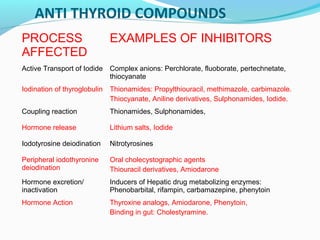


The document discusses thyroid hormones, their biosynthesis, regulation, actions, and peripheral conversion. Some key points: - Thyroid hormones T4 and T3 are synthesized in thyroid follicles from iodine and tyrosine. T4 is the main secretory product while T3 is the biologically active form. - TSH stimulates thyroid hormone synthesis and secretion. T4 is converted to T3 in tissues by deiodinase enzymes. - Thyroid hormones are transported bound to carrier proteins and the free forms enter cells to increase metabolism. - Thyroid hormone levels are regulated by a negative feedback loop involving the hypothalamus, pituitary and thyroid gland.

















































![Advanced Trauma Life Support [ATLS] and Triage](https://cdn.slidesharecdn.com/ss_thumbnails/atlstriage-251212075759-fbe88f4f-thumbnail.jpg?width=640&height=640&fit=bounds)




































