
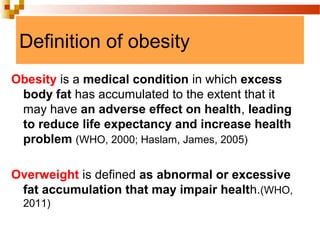




The document discusses obesity as a major public health issue, emphasizing its increasing prevalence, health risks, and economic impact globally and locally. It outlines obesity's definitions, classifications, risk factors, health effects, and treatment options, alongside the community health nursing role in prevention and education. Additionally, research findings are presented, indicating a significant prevalence of overweight and obesity among school children in Jordan.






































![Obesity by bijay [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/obesitybybijayautosaved-200407031519-thumbnail.jpg?width=640&height=640&fit=bounds)





































