Downloaded 177 times

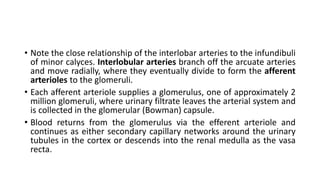
![Vascular anatomy of the ureteropelvic
junction: importance for endopyelotomy
• Today, endopyelotomy is a common procedure for both primary and
secondary UPJO.
• The risk of injuring a large vessel during endopyelotomy can be
greatly reduced or even eliminated if the endourologist understands
and keeps in mind the 3D vascular relationships to the UPJ [44, 45,
51]. This section describes the vascular anatomy of the UPJ and this
should be used to perform endopyelotomy safely and efficiently.](https://image.slidesharecdn.com/renalvascularanatomy-170810190422/85/Renal-vascular-anatomy-38-320.jpg)
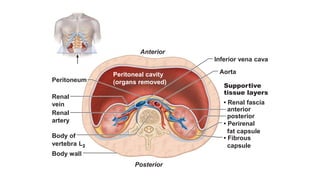
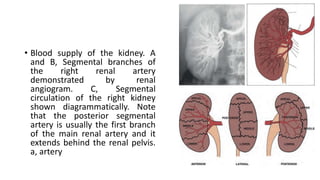
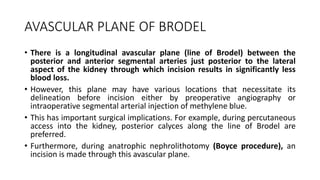
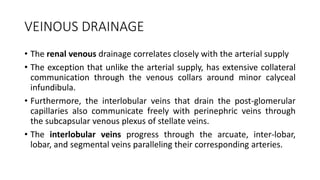
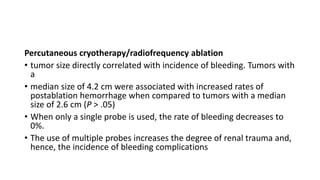
![Figure 6.41
(A) Anterior view of a right kidney
endocast (pelviocalyceal system
together with the intrarenal arteries)
shows a close relationship between
the inferior segmental artery and the
anterior surface of the ureteropelvic
junction (UPJ; arrow). u, ureter. (B)
Anterior view of a right kidney
endocast (pelviocalyceal system
together with the intrarenal veins)
shows a close relationship between a
vein draining the lower pole and the
UPJ (arrow). RV, renal vein; u, ureter
(reproduced from Sampaio and
Favorito [44], with permission).](https://image.slidesharecdn.com/renalvascularanatomy-170810190422/85/Renal-vascular-anatomy-39-320.jpg)


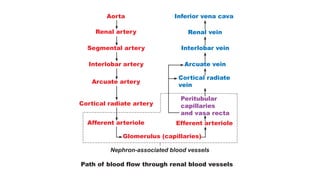
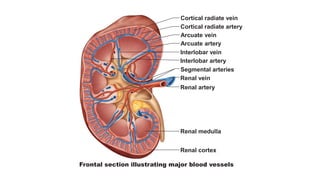
The document discusses renal vascular anatomy and its implications for surgery. It notes that the renal arteries typically enter the kidney through the hilum and branch into segmental arteries that do not anastomose. It also describes variations such as accessory renal arteries. The segmental arteries further branch within the kidney and an avascular plane exists between anterior and posterior branches. Venous drainage parallels the arterial supply. Imaging like CTA can accurately map the vasculature preoperatively to aid surgery. Understanding variations and collateral circulation is important for procedures like donor nephrectomy.












































































