Downloaded 103 times

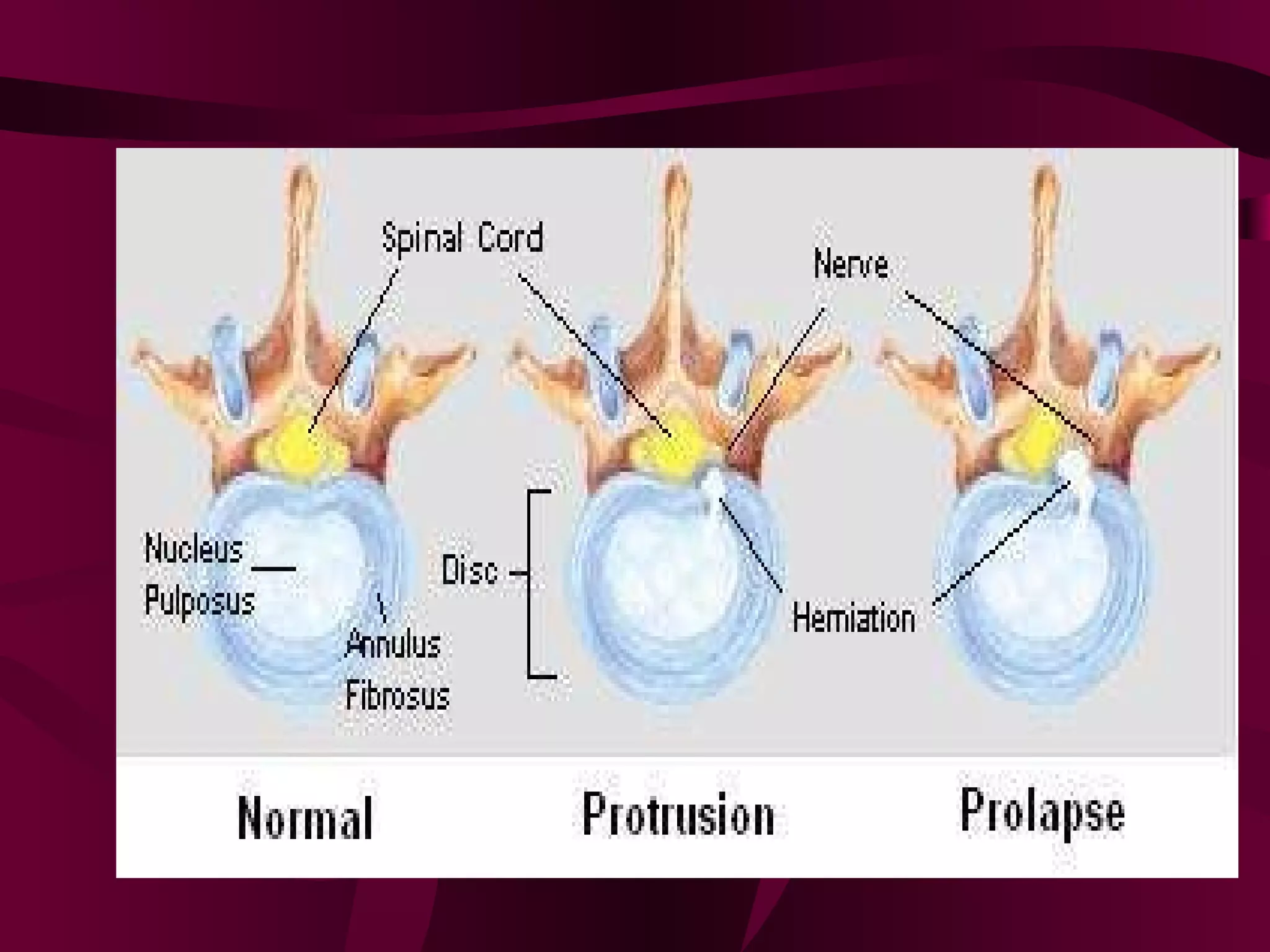
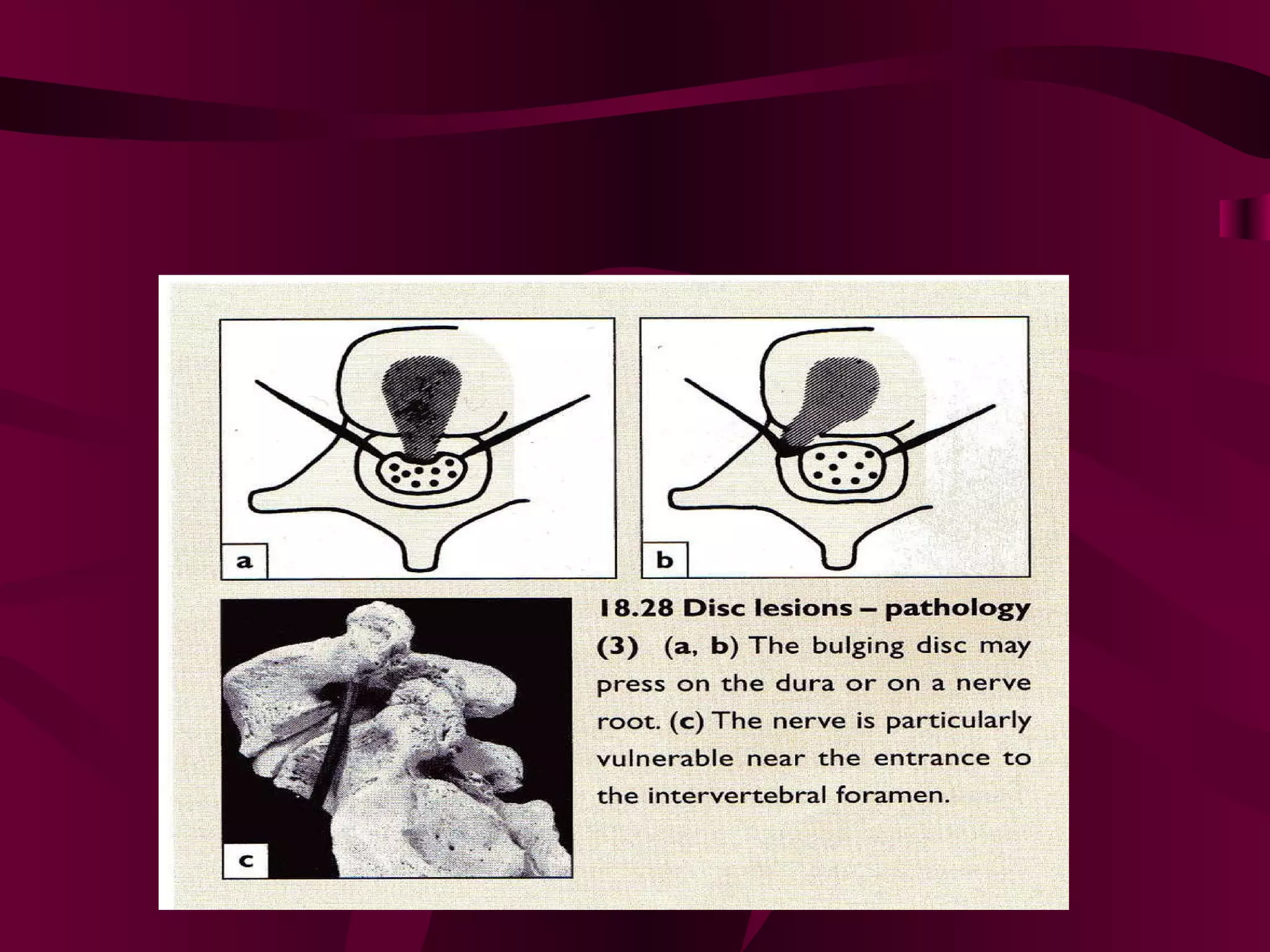
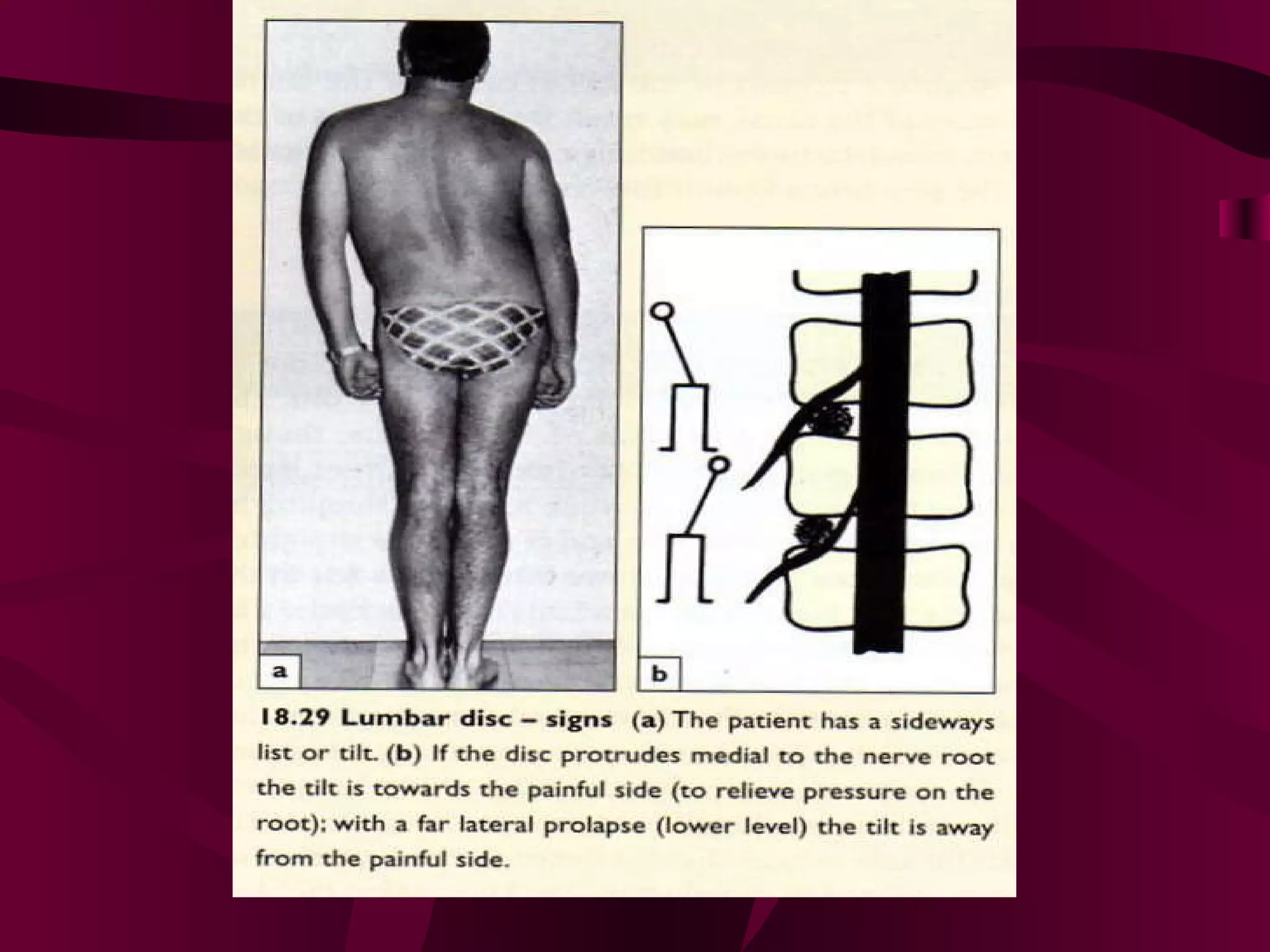
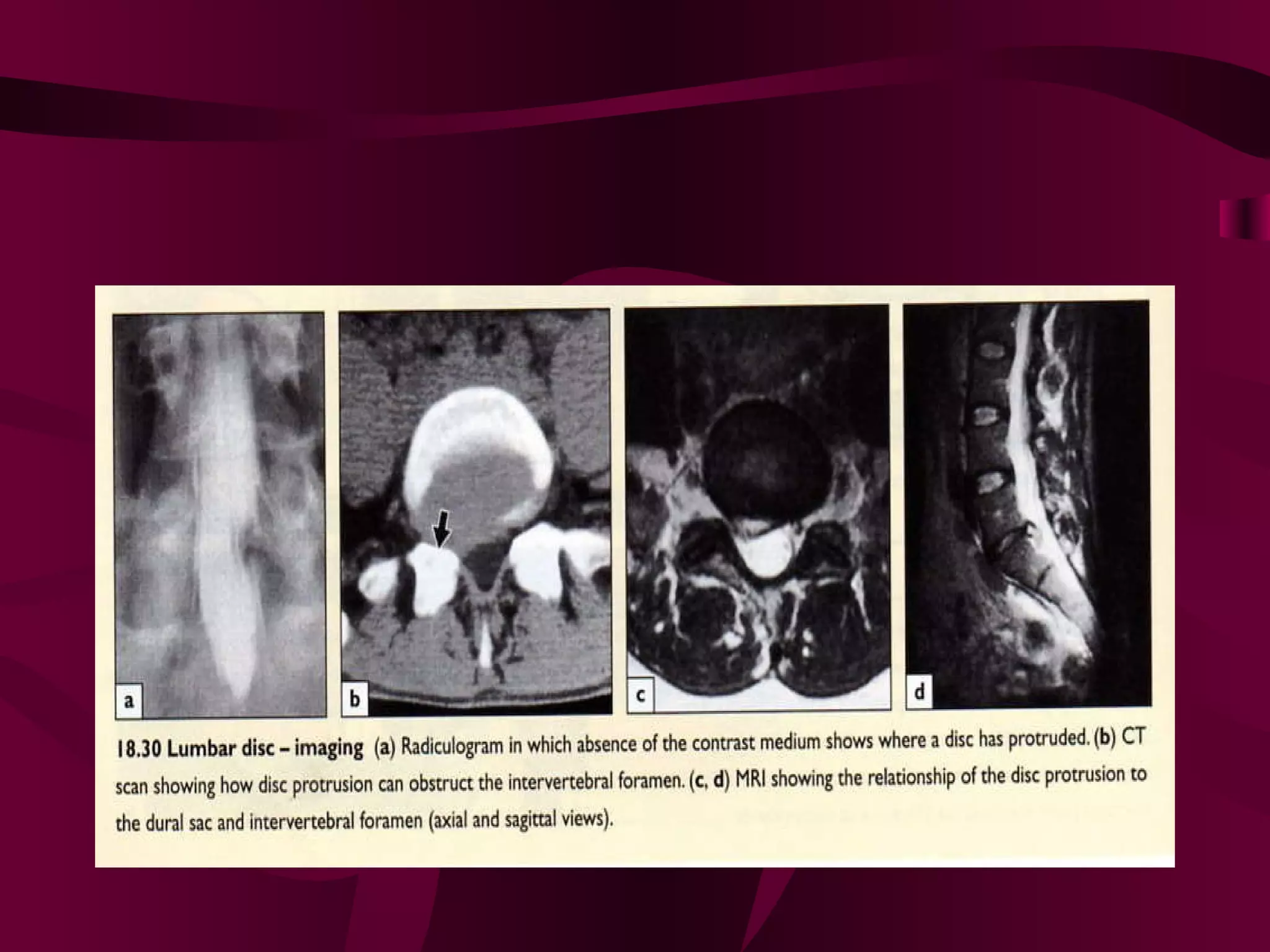










Prolapsed Intervertebral Discs can be caused by chronic degeneration from normal aging or acute disc herniation which causes pain and compression effects on the nerve root. Imaging like x-rays, MRI, and CT scans are used to diagnose the condition. Treatment options include rest, gentle massage, bracing, anti-inflammatory medications, epidural blocks, and surgery like microdiscectomy if conservative treatments fail. Surgical treatment aims to decompress the nerve root while avoiding excessive scarring and early mobilization is emphasized.






















































































