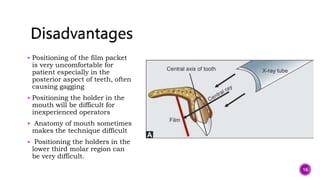
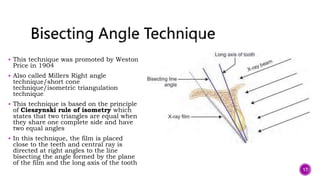
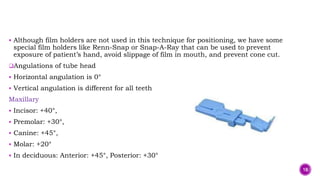
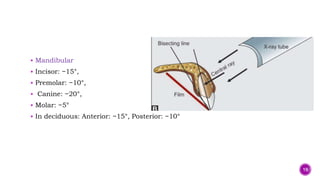
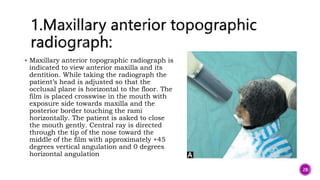
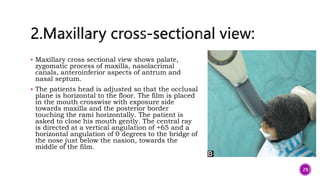
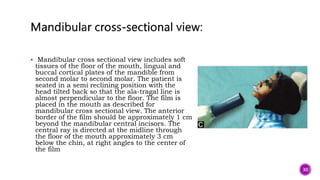
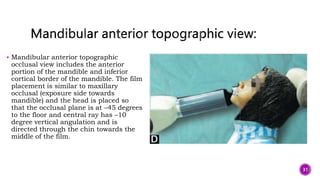
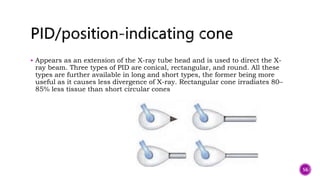
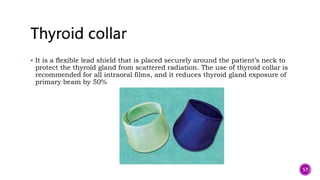
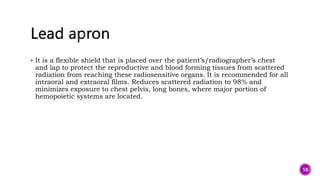
The document discusses diagnostic radiography techniques used in pediatric dentistry. It begins with an introduction and overview of the importance of radiographs in diagnosis and treatment planning. It then covers the history of x-rays and components of x-ray machines. The document discusses various intraoral and extraoral radiographic techniques including paralleling, bisecting angle, bitewing, occlusal, and panoramic techniques. It provides details on positioning, advantages, and limitations of each technique. Radiation protection and behavioral considerations are also covered.