



















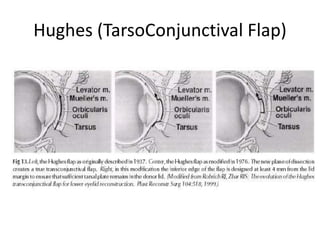







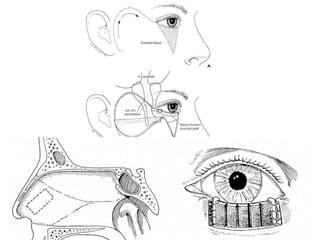









Lower eyelid reconstruction aims to re-establish a functional eyelid with adequate protection of the eyeball and reasonable cosmesis. Direct closure can be used for up to 30-40% defects in younger patients with eyelid laxity. The Hughes procedure uses a tarso-conjunctival flap to reconstruct large posterior lamella defects but requires a second stage for anterior lamella coverage. The Tenzel slide uses a semicircular musculocutaneous flap to reconstruct large anterior lamella defects but requires posterior lamella coverage. Free tarsal grafts can be used to replace the posterior lamella while the anterior lamella is covered with a myocutaneous advancement flap.










































































