Downloaded 135 times
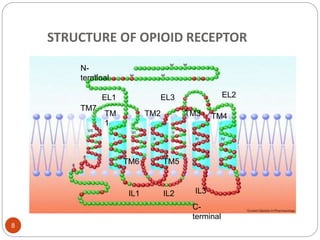
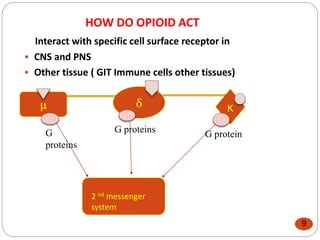
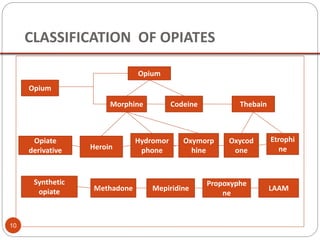
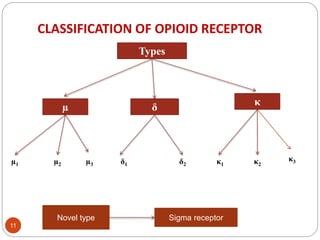
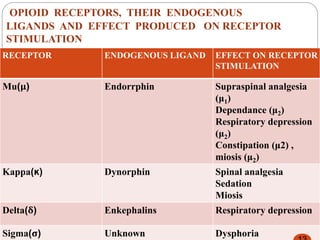
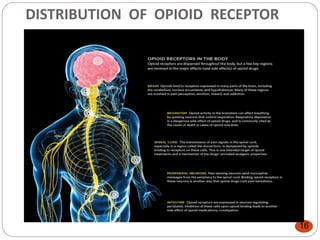
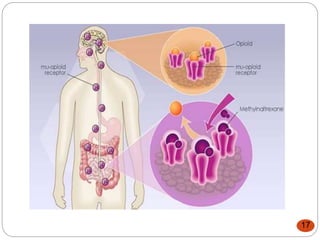
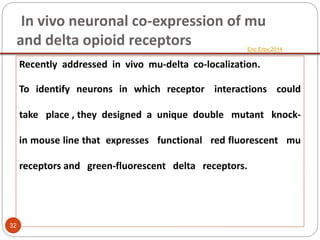
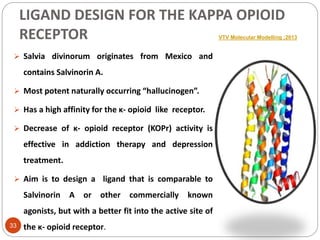

This document provides an overview of opioid receptors including: - A brief history of opioid research from ancient times to the 1970s identification of opioid receptors. - The structure of opioid receptors including their classification into mu, delta, and kappa types along with endogenous ligands and effects. - The mechanism of action of opioids through G-protein coupled receptors and cellular responses. - The distribution of opioid receptors in the central and peripheral nervous systems. - Recent advances in understanding the role of opioid receptors in various physiological functions like neuroprotection, immune response, and more. - Studies on designing new ligands for the kappa opioid receptor and on in vivo co-expression of mu and delta opioid receptors.








































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














