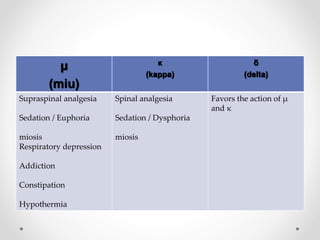
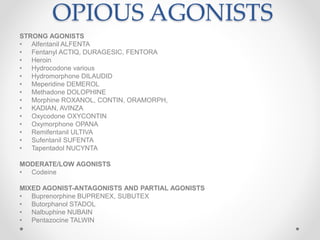
This document discusses opioids, which are drugs that bind to opioid receptors in the central nervous system to produce analgesic, calming, sedative, and euphoric effects. It describes endogenous opioids like endorphins and exogenous opioids extracted from opium or produced synthetically. The three main types of opioid receptors are mu, kappa, and delta. Representative opioid drugs are discussed, including morphine, heroin, methadone, fentanyl, buprenorphine, and antagonists like naloxone. The pharmacological effects, indications, and side effects of various opioids are outlined.