Download as PPSX, PPTX
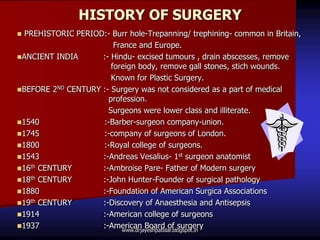


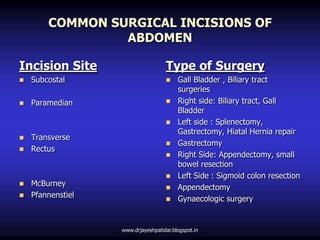





The document discusses the history and development of surgery from prehistoric times to the present. It covers key figures and advances such as the first surgeon anatomist Andreas Vesalius in the 16th century, Ambroise Pare being considered the father of modern surgery, and John Hunter founding surgical pathology. The document also outlines the purposes and types of surgery as well as common abdominal incisions and the organization and layout of operating theaters. It provides principles for planning the physical layout of operating rooms and discusses perioperative patient care from the preoperative to intraoperative to postoperative phases.