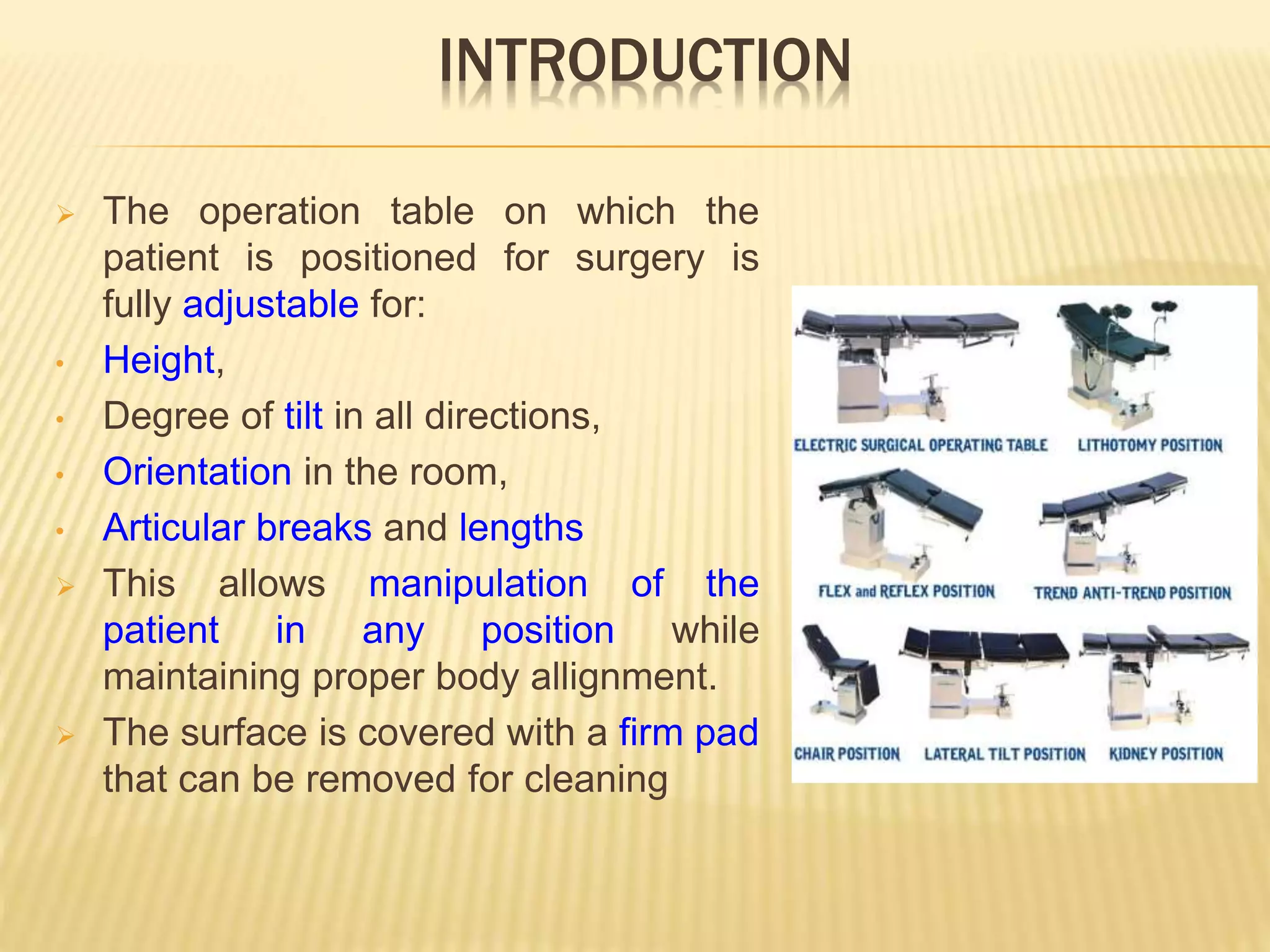
1. The operating room table is fully adjustable to position patients in various surgical positions and orientations. It has movable sections, articulating joints, and tilt capabilities to manipulate the patient as needed.
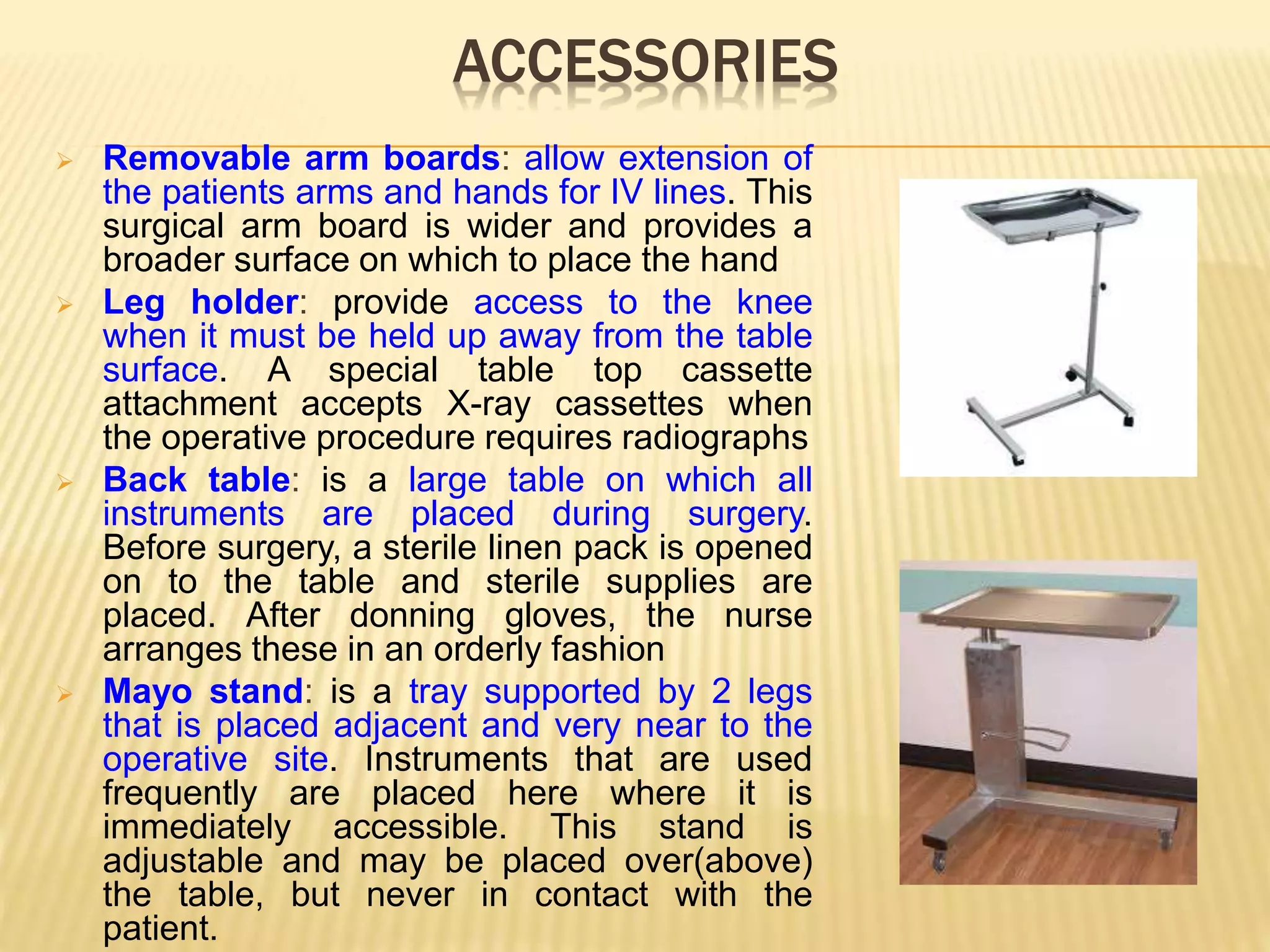
2. Accessories like armboards, leg holders, and overhead tables provide support and access around the patient. The table also has features like smooth contours, radiolucency, and electrical or hydraulic controls for adjustments.
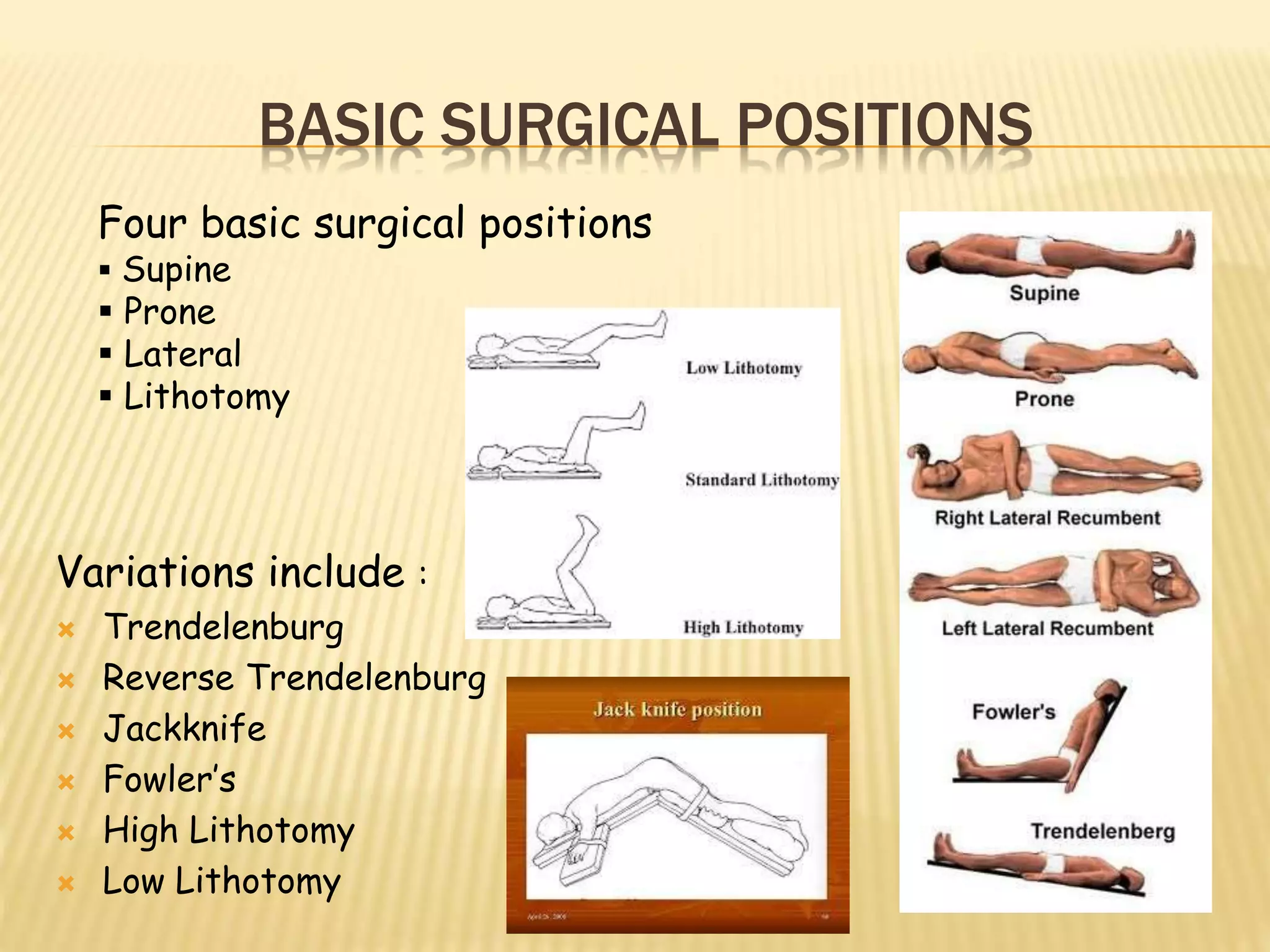
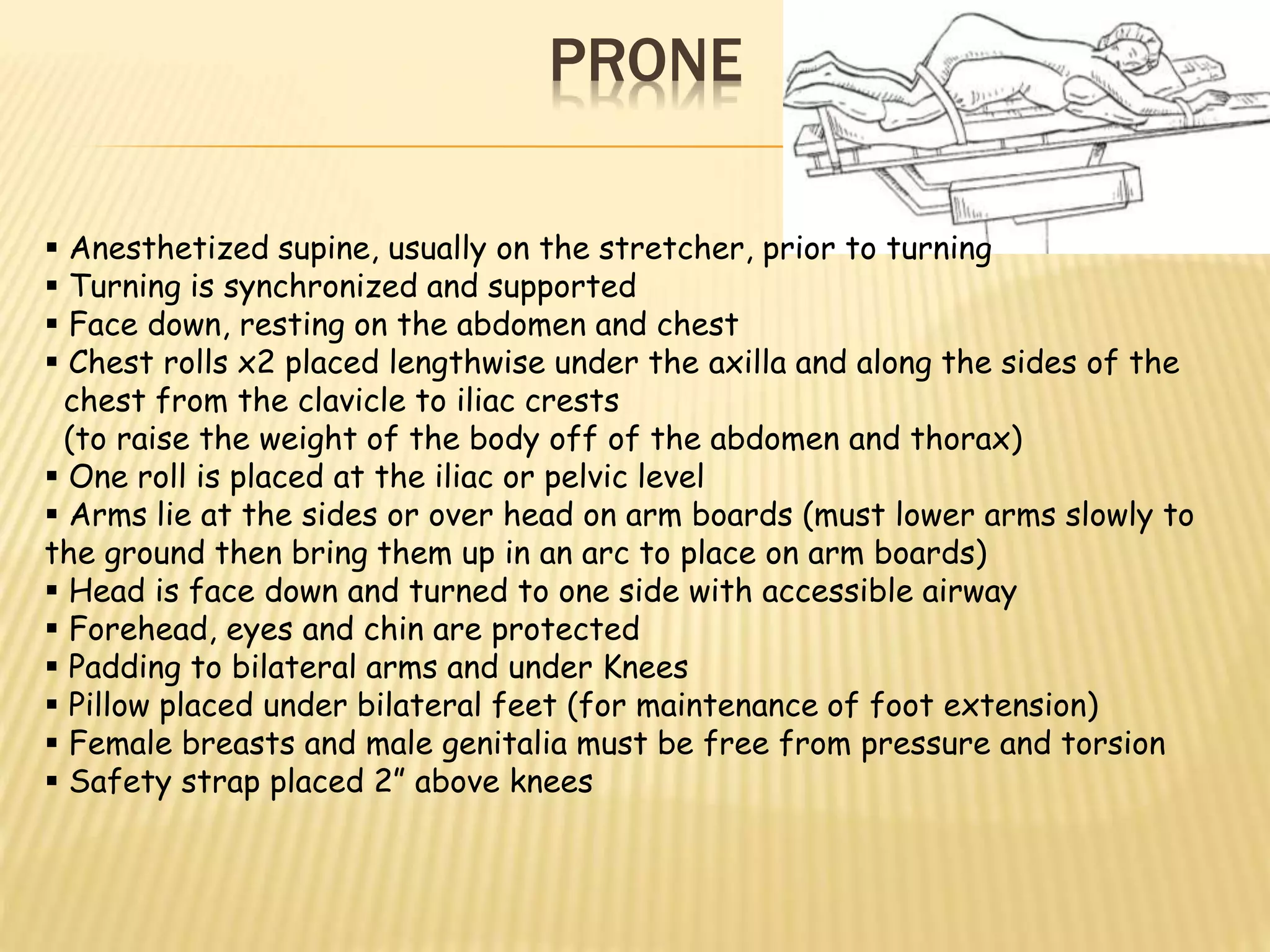
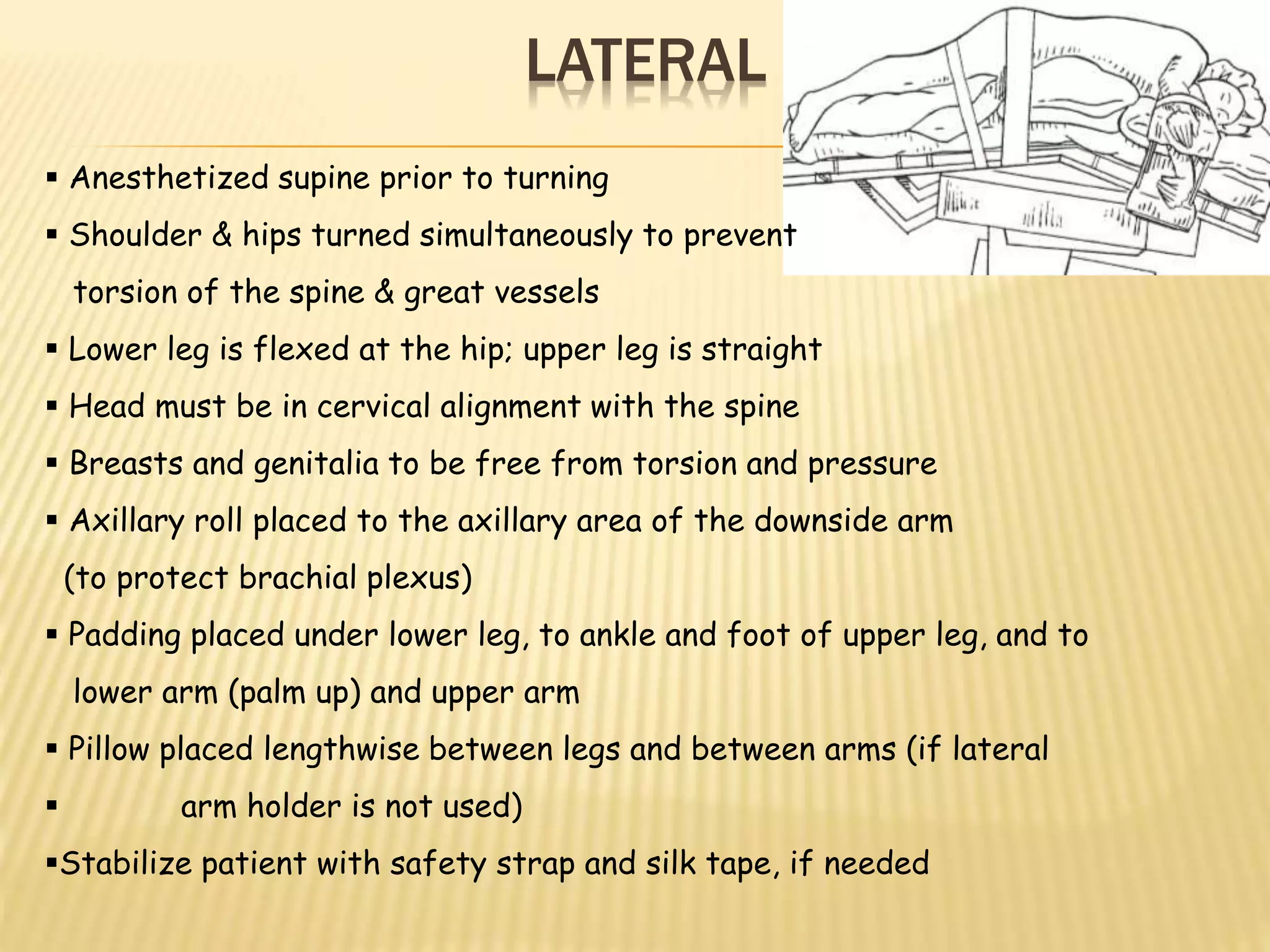
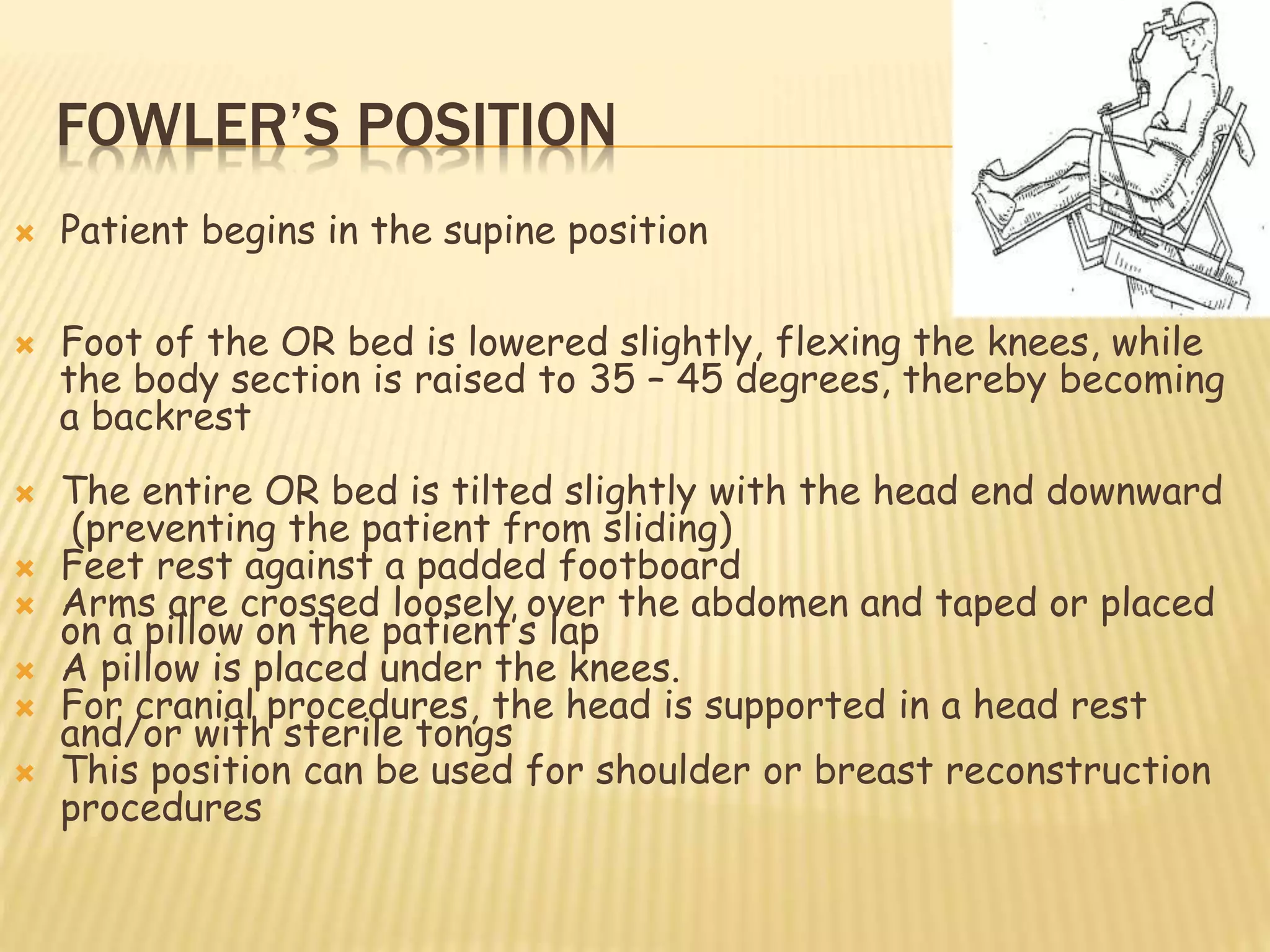
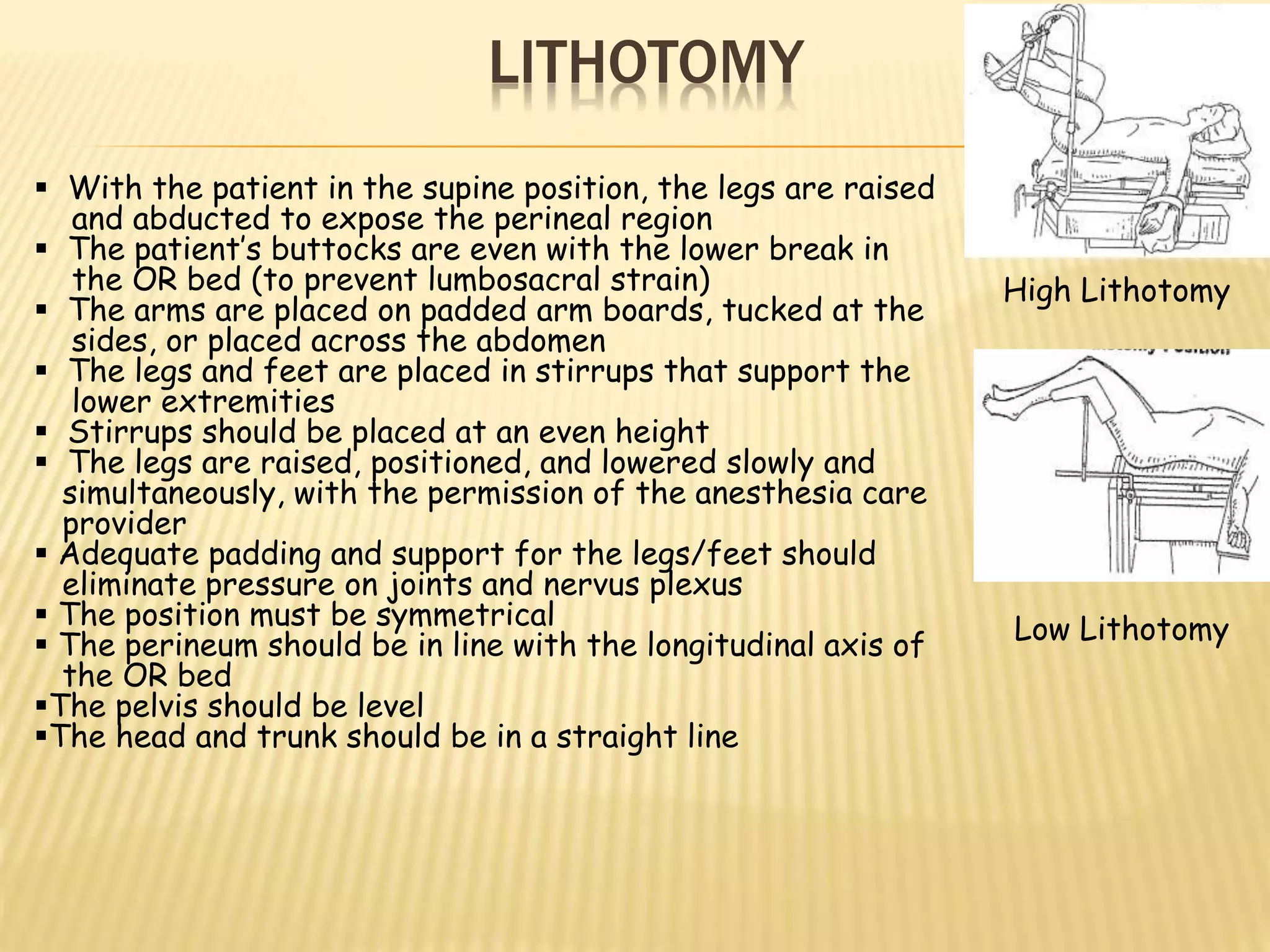
3. Proper positioning is important for patient safety, surgical access, and physiological needs. It prevents pressure points, maintains circulation and breathing, and positions anatomical structures for procedures. Common positions include supine, prone, lateral, lithotomy and their variations.