






































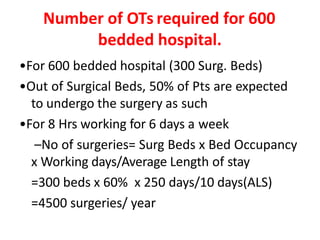








































































The document provides a comprehensive overview of the operation theater (OT), detailing its definition, purpose, types of surgeries, and the importance of maintaining a sterile and controlled environment. It discusses the advantages and disadvantages of inpatient and outpatient surgeries, including the necessary facilities and zoning within the OT for optimal functionality. Key elements of OT planning such as design parameters, air supply methods, and safety measures are also emphasized to ensure effective surgical outcomes.






















































































