1:2
▪ Night 1:4
❑ICU Matron
❑Nursing orderly
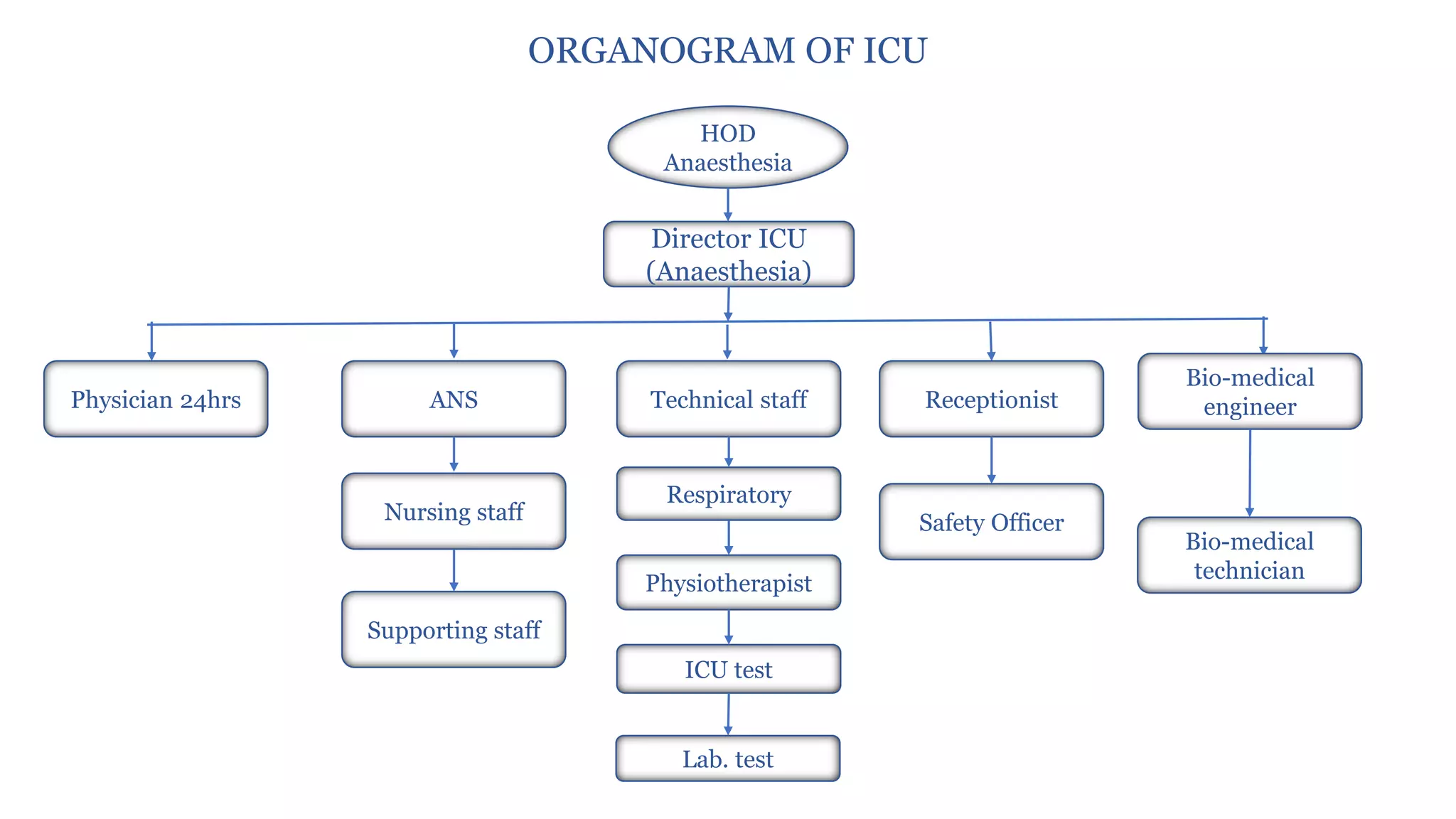
➢ Medical Staff
❑Consultant: 1:4 beds
❑Resident: 24 hrs
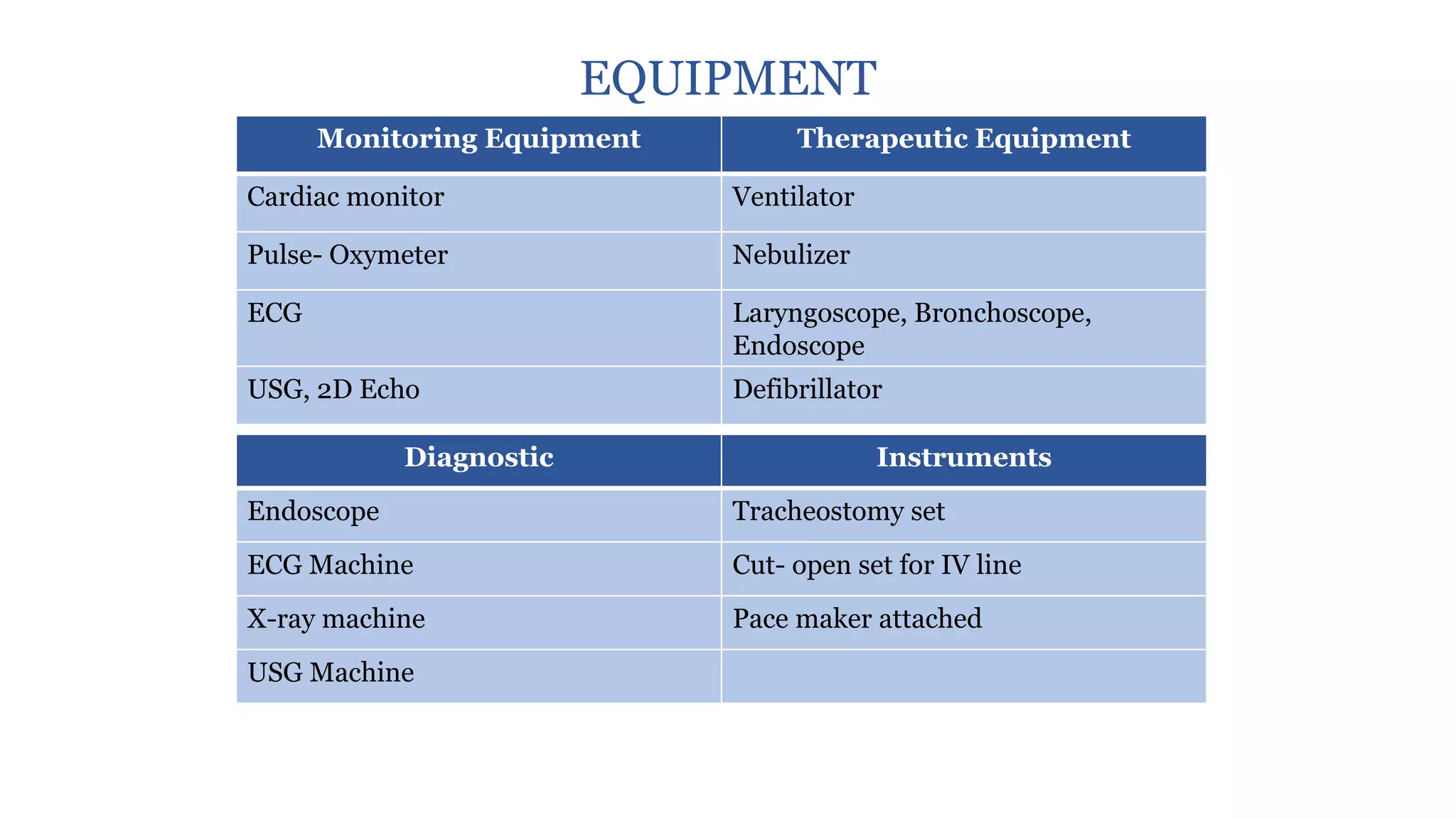
➢ Technical Staff
❑Respiratory therapist
❑ECG/Echo technician
❑Lab technician
❑X-ray technician
➢ Ancillary Staff
❑Housekeeping
❑Dietician
❑Physiotherapist
❑Social worker
❑Pharmacist
❑Bio-medical engineer
❑Safety officer














































































![4._LAY_OUT_OF_CRITICAL_CARE_UNIT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/4-250506110215-46b0d8f2-thumbnail.jpg?width=640&height=640&fit=bounds)





















