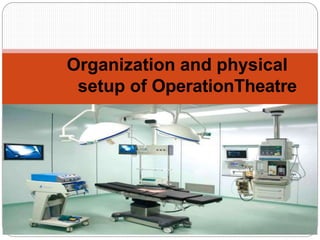
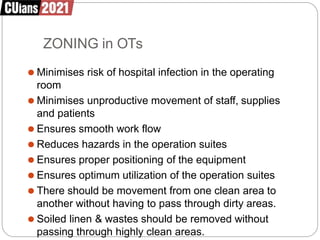
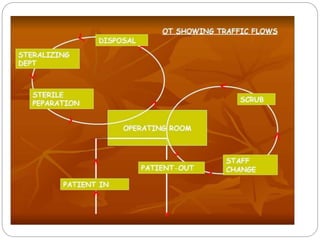
The document discusses the organization and physical setup of an operation theatre. It describes key aspects of an operation theatre including its purpose of carrying out surgical procedures under aseptic conditions. It covers types of surgeries, advances in surgery techniques, objectives, components of an operation theatre complex, factors in determining the number of operation theatres, design considerations, zoning, and policies on cleaning techniques for maintaining aseptic standards.














![Infection Control Guidelines for Laundry Services [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforlaundrycompatibilitymode-131231001333-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)






























































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)
![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)














