Downloaded 158 times
![GENERAL PROPERTIES OF VIRUS
Virus is the smallest known micro organism
[10nm-300nm]
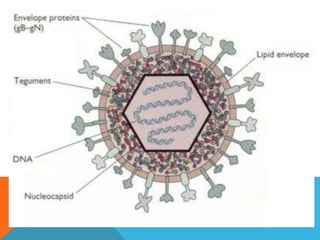
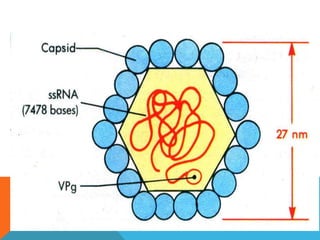
It consists of a nucleic acid core(RNA/DNA)
surrounded by a protein coat.
They are metabolically inert and hence requires
living cells to survive and replicate.
The protein coat which is antigenic in nature is
called a ‘Capsid’ and together with the nucleic
acid is termed as ‘Virion’. The capsid is made up
of protein subunits called as ‘Capsomeres’](https://image.slidesharecdn.com/ocularvirology-141209092533-conversion-gate02/85/Ocular-virology-2-320.jpg)

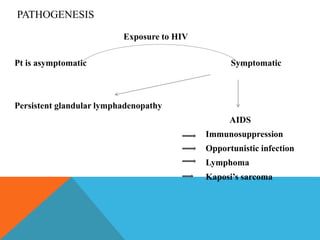





This document discusses various viruses that can cause eye infections or diseases. It provides details on the general properties of viruses, then examines specific viruses like adenovirus, herpes simplex virus, herpes zoster, cytomegalovirus, pox viruses, picornaviruses, paramyxoviruses, measles, rubella and HIV. For each virus, it describes the viral structure, transmission, signs and symptoms of ocular infection, laboratory diagnosis and treatment approaches.














































![Socialization[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/socialization1-ppt-120131084221-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




















































