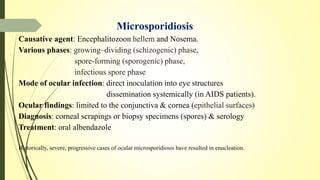
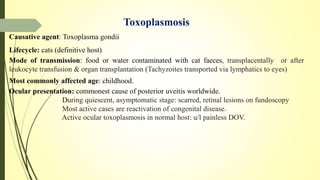
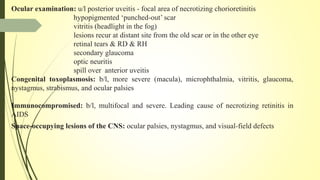
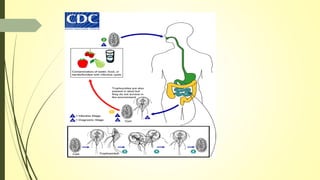
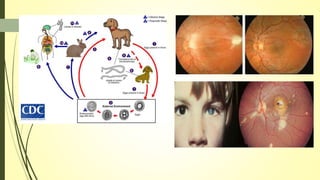
This document summarizes various parasitic diseases that can involve ocular structures. It discusses the causative agents, life cycles, modes of transmission, common ocular findings, diagnosis, and treatment options for a wide range of systemic parasitic infections that may result in direct infection, inflammation, or other pathology in the eye. These include infections caused by microsporidia, various protozoa, nematodes, cestodes, trematodes, and pentastomes. Common ocular manifestations discussed include uveitis, retinitis, optic neuritis, and other inflammatory conditions or space-occupying lesions of the eye.


























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














