Downloaded 383 times
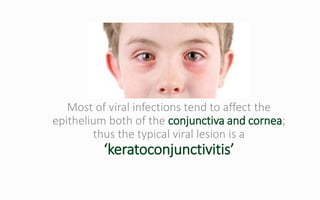
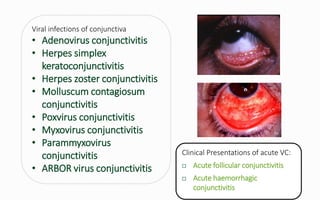

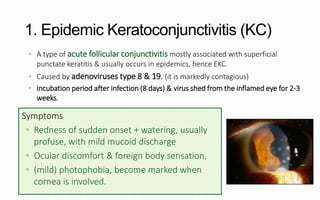





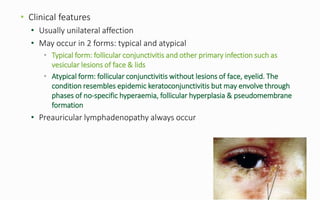
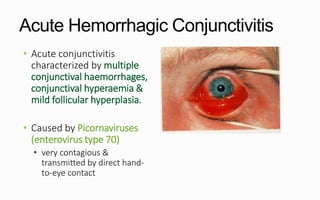
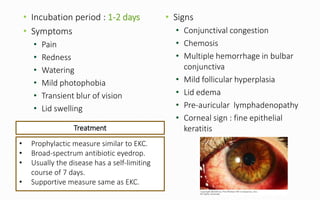
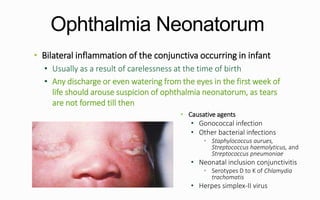


Viral conjunctivitis is caused by various viruses that infect the conjunctiva. The most common types are adenoviral conjunctivitis, caused mainly by adenovirus types 8 and 19, and herpes simplex conjunctivitis caused by HSV-1. Adenoviral conjunctivitis presents with redness, watering, follicles and can cause punctate keratitis if the cornea is involved. Treatment focuses on supportive care and antibiotics to prevent secondary infections. Acute hemorrhagic conjunctivitis is caused by enterovirus 70 and presents with redness, watering, hemorrhages and follicles. Ophthalmia neonatorum can be caused by gon
































































































