Downloaded 211 times

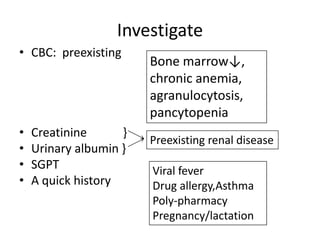



This document summarizes the use of NSAIDs in clinical orthopaedic practice. It discusses the mechanisms of inflammation and pain, the role of prostaglandins, and the modes of action of NSAIDs. It describes the benefits of NSAIDs including analgesia and anti-inflammatory effects. However, it also outlines the various toxicities of NSAIDs including risks of gastrointestinal bleeding, acute renal failure, myocardial infarction, skin reactions, and bone marrow suppression. It provides guidance on identifying patients at higher risk and investigating them before committing to NSAID treatment. The document emphasizes starting low, going slow, stopping to assess, and monitoring patients on NSAIDs.




































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






