Downloaded 67 times
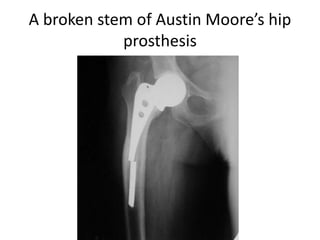
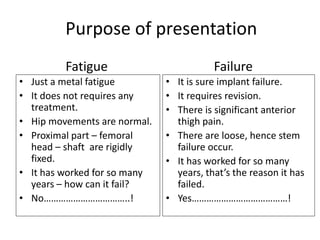
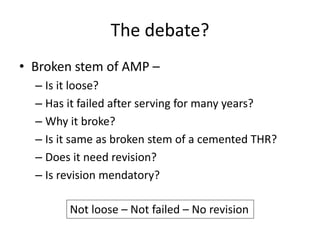



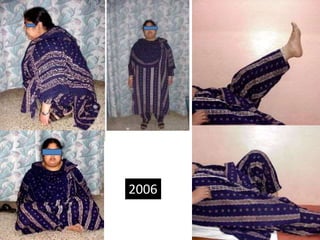







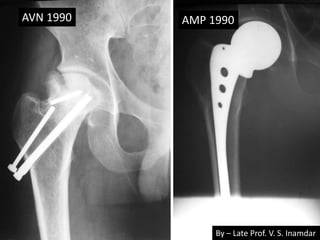
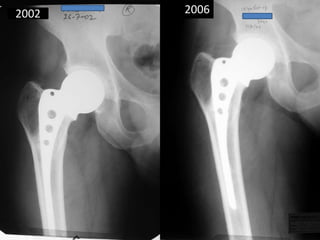












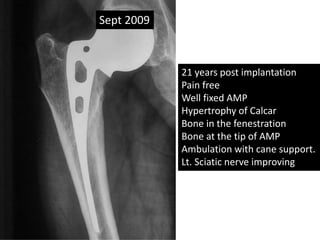


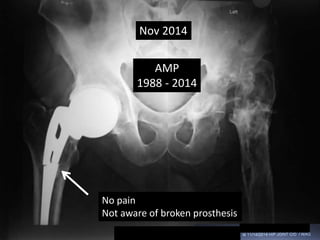
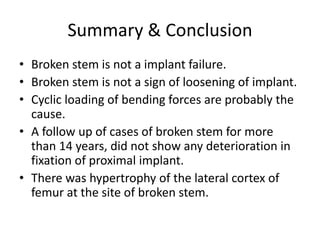

The document discusses the phenomenon of broken Austin Moore hip prostheses, suggesting that stem fractures are largely a result of metal fatigue rather than implant failure. Observations from multiple cases indicate that broken stems do not typically require revision, as they often remain well-fixed without signs of loosening. The findings highlight the importance of understanding the mechanical forces at play and their implications for patient care and the longevity of hip prostheses.































![Thigh pain after total hip arthroplasty [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/thighpainaftertotalhiparthroplastyautosaved-200110172905-thumbnail.jpg?width=640&height=640&fit=bounds)























































