Downloaded 10 times
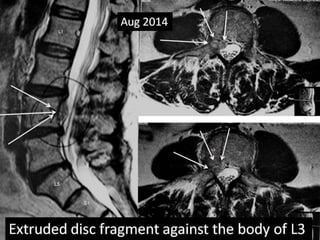




A 40-year-old male presented with acute right knee pain and frequent falls over the past week without a history of trauma. Examination found reduced right knee reflex but no other abnormalities. MRI revealed an L3-L4 disc extrusion. Though the patient's pain was in the knee, the neurological exam suggested radiculopathy and MRI confirmed lumbar disc disease, demonstrating that knee pain can originate from the spine. Conservative treatment was recommended given minimal deficits and low risk of progression.






























![This week cases [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thisweekcasesautosavedautosaved-230219111030-ff5d96f7-thumbnail.jpg?width=640&height=640&fit=bounds)
























































