Downloaded 15 times





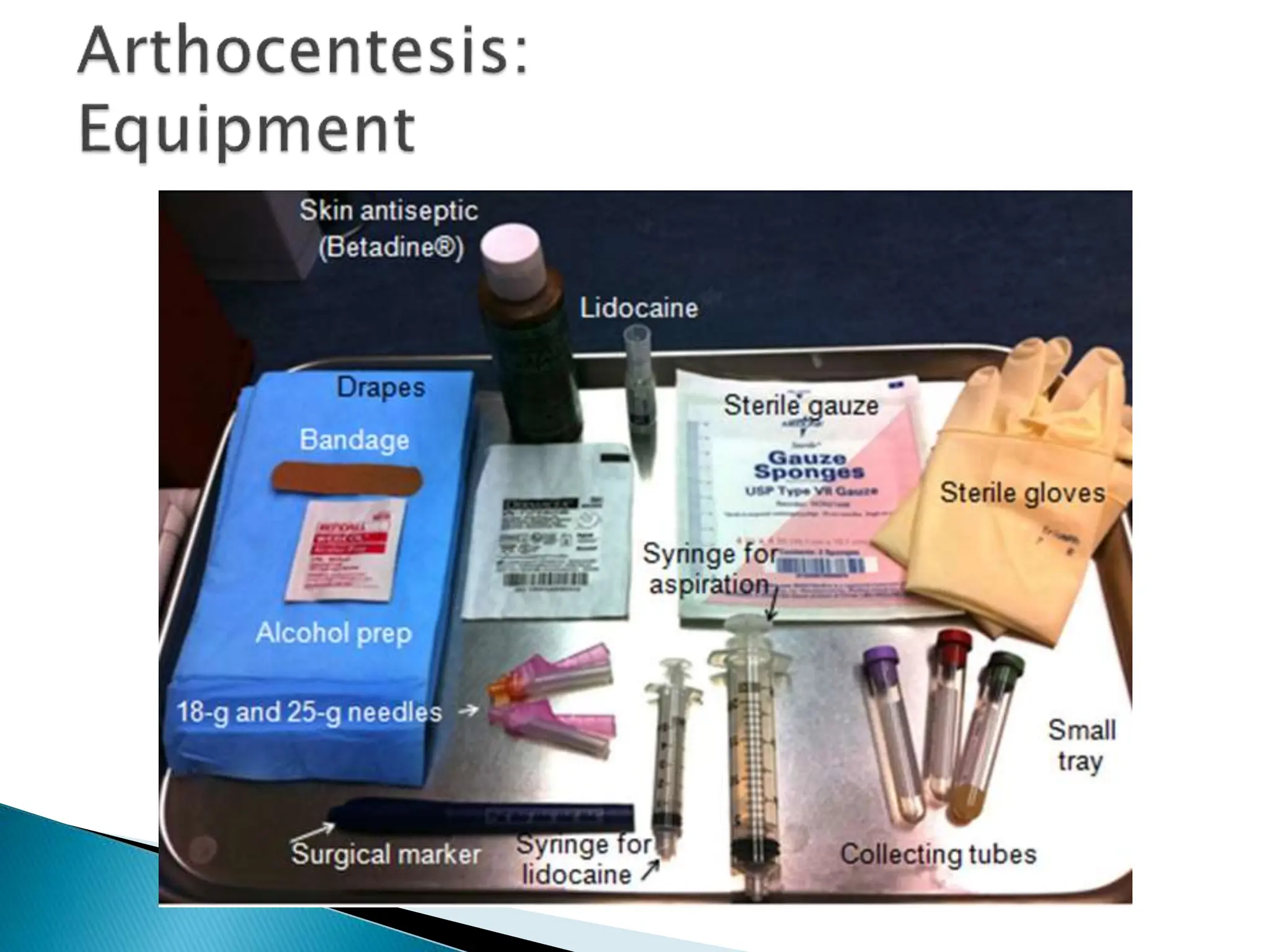


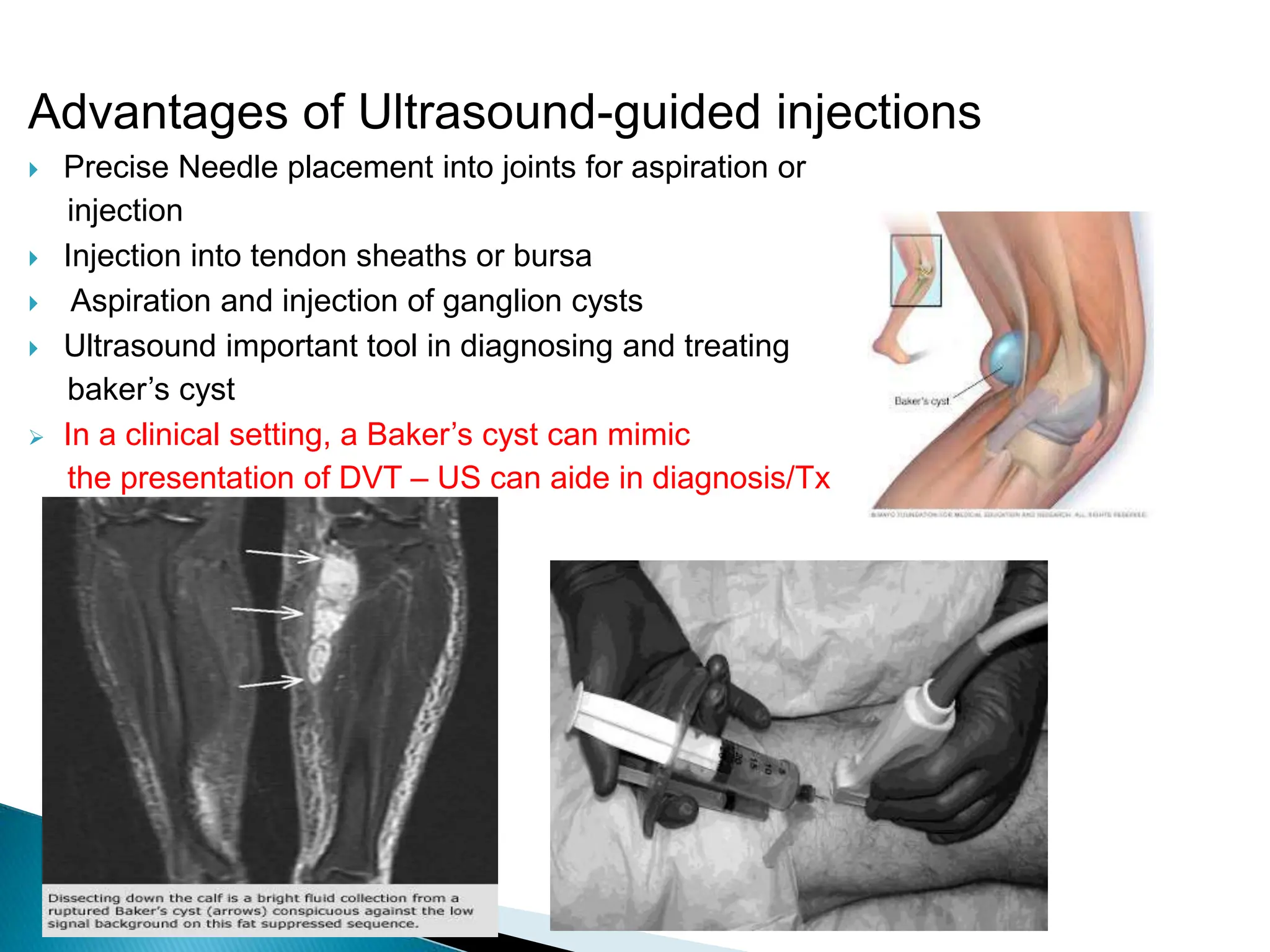

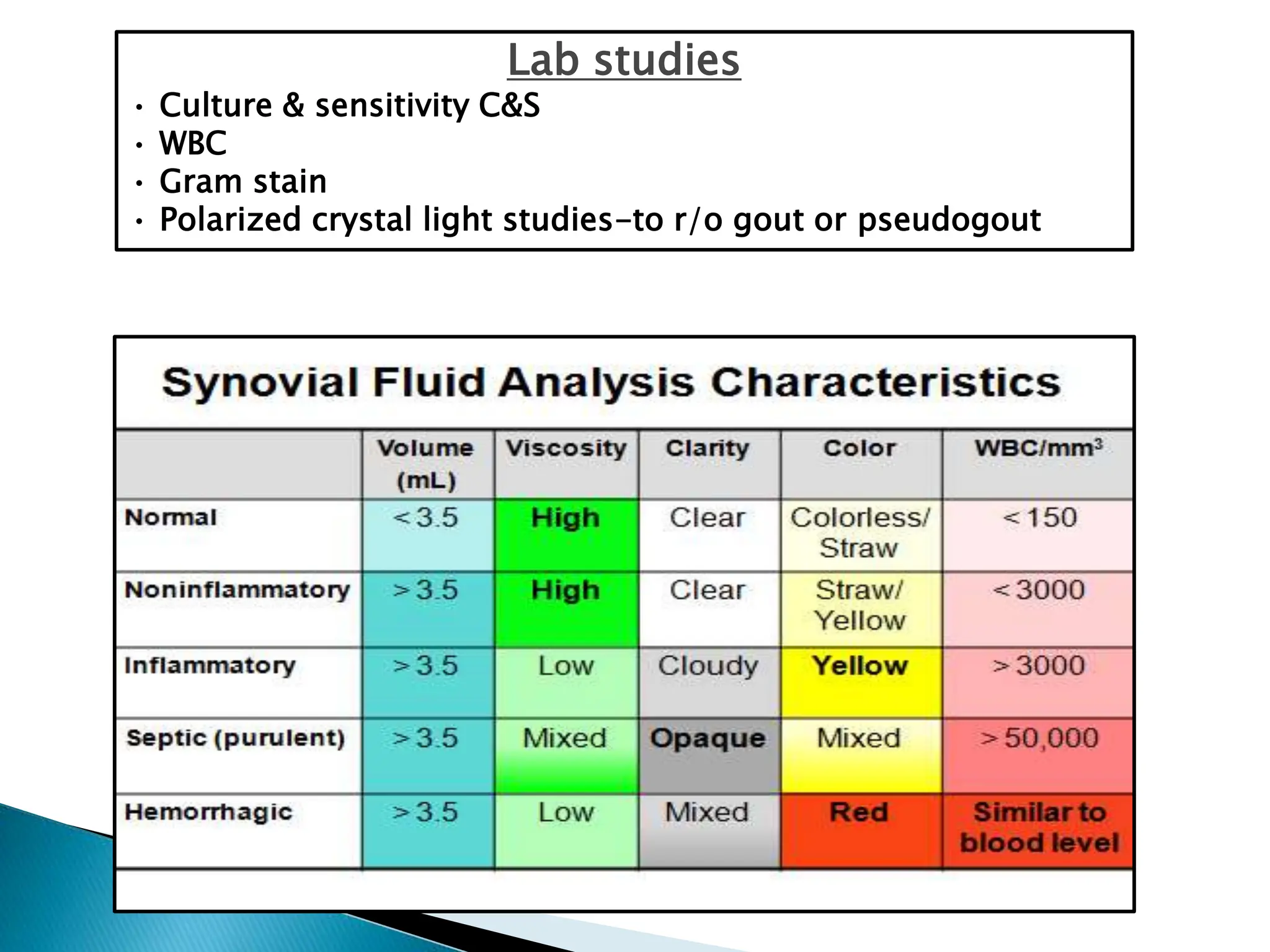










This document discusses the evaluation and management of joint pain. It begins by outlining the important aspects of history and physical exam for joint pain. Common etiologies of joint pain include trauma, infection, inflammatory conditions like gout, pseudogout, and arthritis. Joint aspiration is important for diagnosis and can help differentiate infectious from non-infectious causes. Treatment depends on the underlying cause but may include NSAIDs, colchicine, corticosteroids, or urate-lowering drugs. Proper technique for arthrocentesis and injections is demonstrated.










































































