Downloaded 14 times

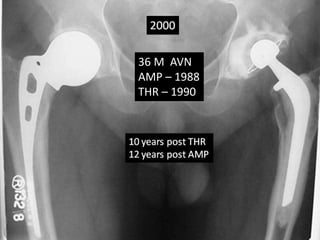
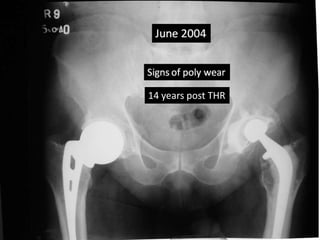


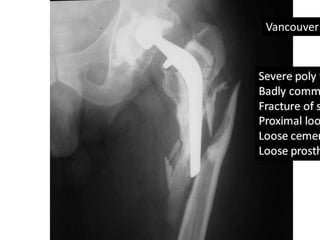





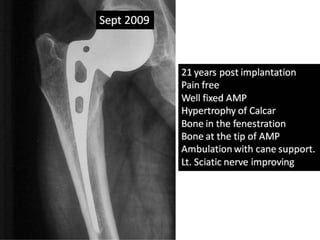


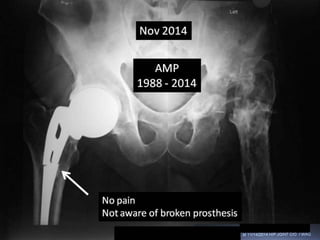
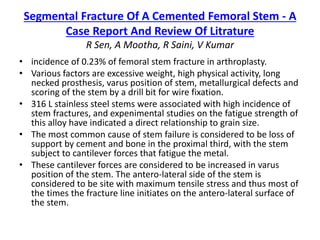

This case report describes a 36-year-old male who underwent an AMP for bilateral avascular necrosis of the hips in 1988. He later required a total hip replacement on the left side in 1990. In 2009, following a traffic accident, he suffered a Vancouver B3 peri-prosthetic fracture requiring revision surgery with a Mennen plate and Solution stem. In 2012, a crack was discovered in the original AMP stem, showing signs of metal fatigue after 24 years. The AMP stem had stood the test of time without causing pain.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




