Downloaded 23 times









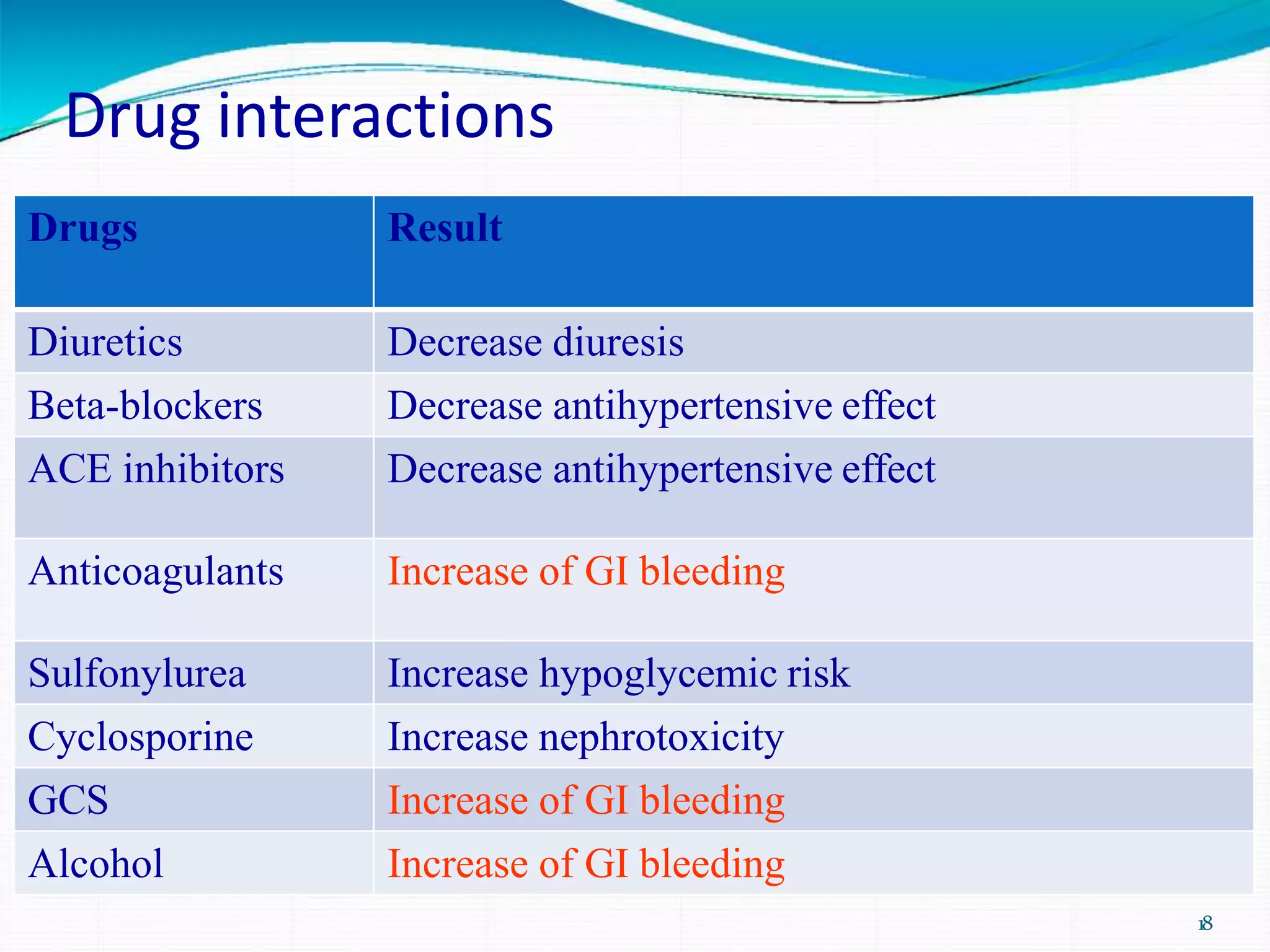









NSAIDs have analgesic, antipyretic and anti-inflammatory properties. They work by inhibiting cyclooxygenase (COX) enzymes and reducing prostaglandin production. NSAIDs are classified as nonselective COX inhibitors like aspirin, preferential COX-2 inhibitors like nimesulide, or selective COX-2 inhibitors like celecoxib. Common adverse effects include gastrointestinal irritation. NSAIDs are used to treat pain, fever, and inflammation conditions like arthritis.



















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


