Downloaded 44 times

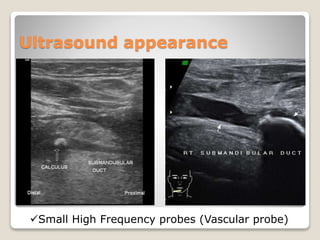


A 45-year-old female presented with sudden pain and swelling in the right cheek, diagnosed with sialolithiasis after imaging revealed a 1.7mm stone in the right parotid gland. The patient received IV pain relief and was discharged with medications and follow-up instructions. Clinical management included hydration, warm compresses, and analgesics, emphasizing the need for potential follow-up if symptoms persisted.





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








