Downloaded 1,660 times

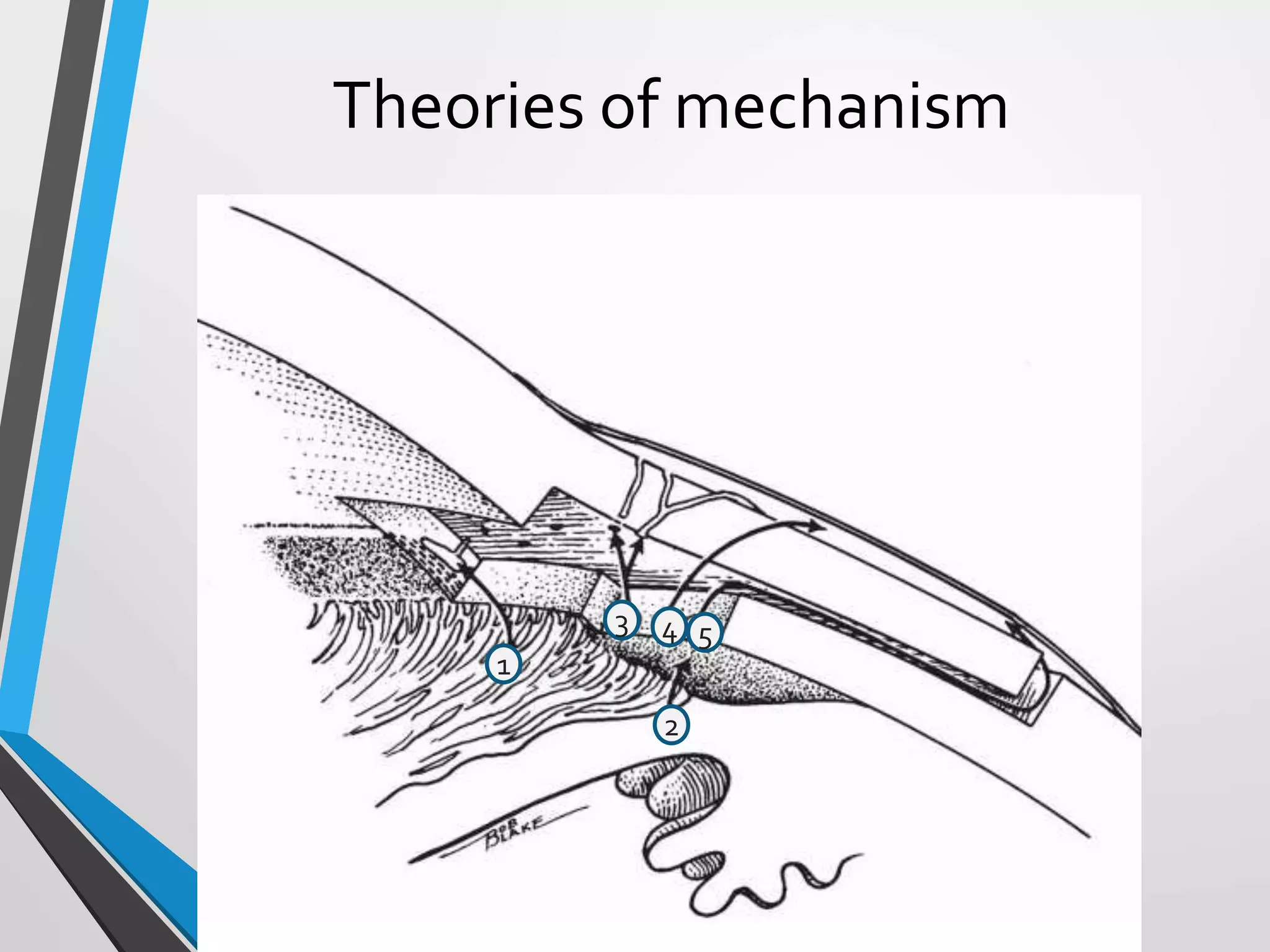





















































































Trabeculectomy is the gold standard glaucoma surgery for lowering intraocular pressure. It involves creating a fistula between the anterior chamber and subconjunctival space to bypass the trabecular meshwork. Complications include hypotony from overfiltration, flat or shallow anterior chambers, elevated pressure, hemorrhage, and infection. Careful surgical technique and postoperative management can help prevent or address complications and optimize outcomes.








































![Adult glaucoma surgery da luz, freitas maria [srg]](https://cdn.slidesharecdn.com/ss_thumbnails/adultglaucomasurgery-daluzfreitasmariasrg-150513044555-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)

























