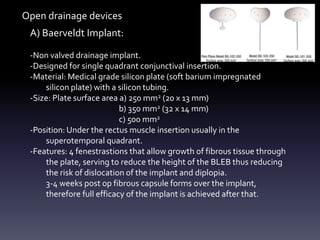
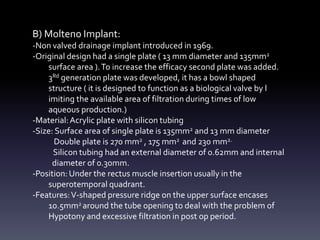
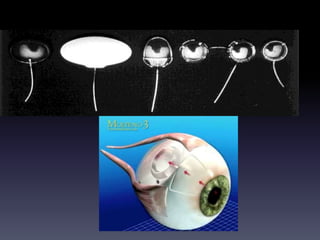
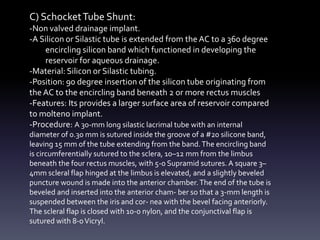
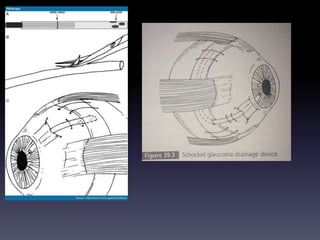
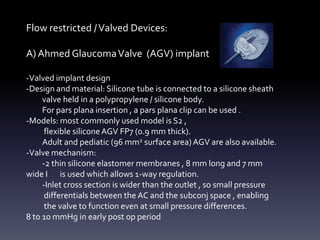
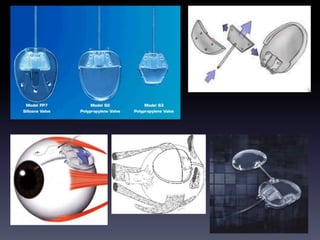
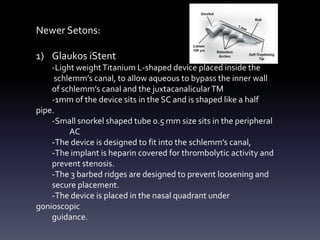
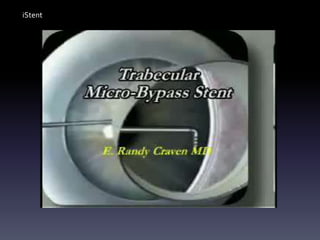
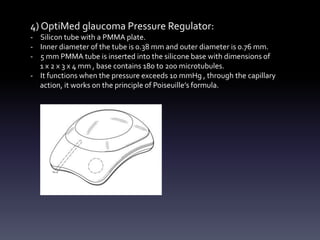
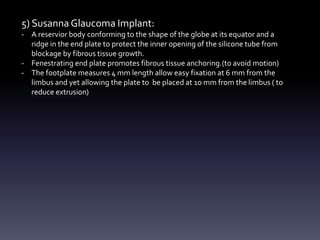
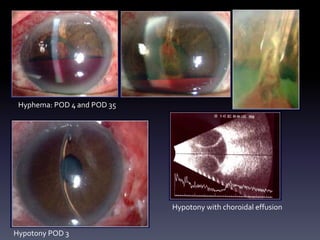
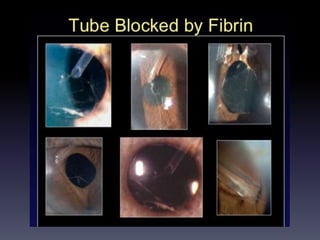
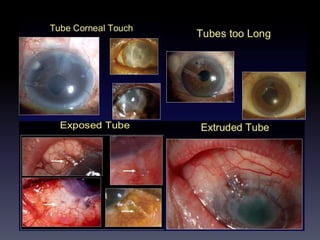
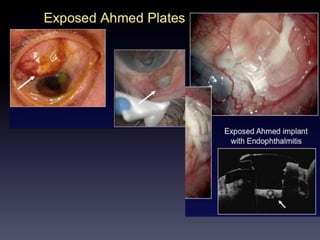
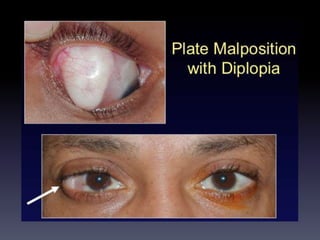
The document discusses glaucoma drainage device (GDD) surgery. It describes the physiology of drainage implants, which involve a silicone tube extending from the anterior chamber to a plate beneath the conjunctiva. A fibrous capsule forms around the external portion of the implant. The document discusses various GDD designs including open-tube devices like the Baerveldt implant, flow-restricted devices like the Ahmed Glaucoma Valve, and newer devices like the iStent. Complications of GDD surgery and the indications for the procedure are also outlined.




































![Glaucoma drainage devices[1]](https://cdn.slidesharecdn.com/ss_thumbnails/glaucomadrainagedevices1-170104084412-thumbnail.jpg?width=640&height=640&fit=bounds)



































