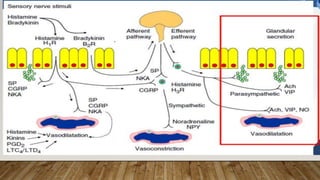
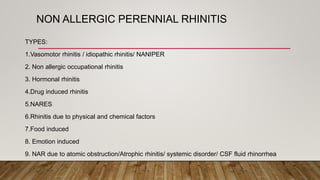
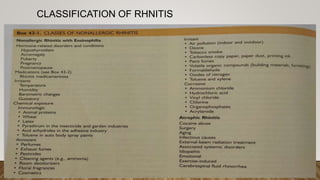
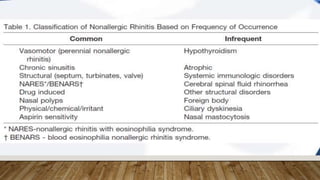
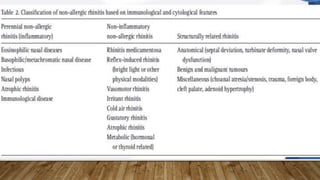
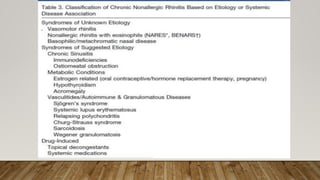
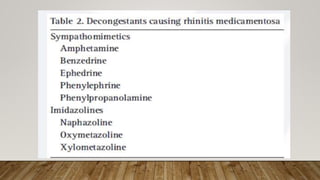
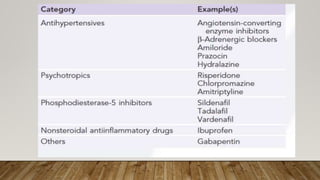
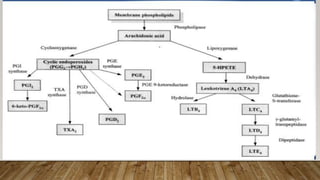
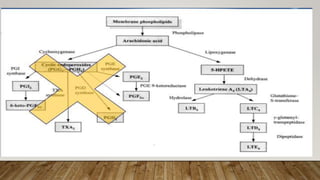
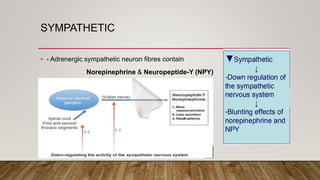
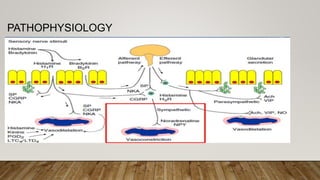
This document provides information about non-allergic rhinitis (NAR), including its various types and causes. It discusses vasomotor rhinitis as the most common form of NAR, accounting for at least 2/3 of cases. Other types include occupational rhinitis, hormonal rhinitis, food-induced rhinitis, and drug-induced rhinitis. It also describes NARES (non-allergic rhinitis with eosinophilia syndrome) which is characterized by nasal eosinophilia without evidence of allergy. The pathophysiology of NAR involves neurogenic mechanisms mediated by sensory C fibers and the autonomic nervous system leading to nasal inflammation and symptoms.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

