Downloaded 156 times

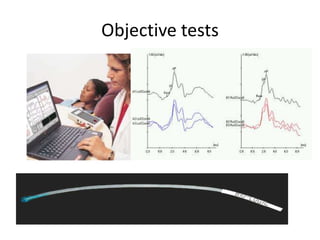
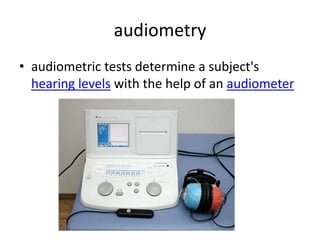
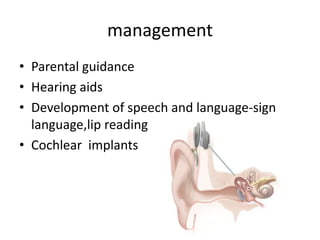

The document discusses various causes and types of deafness in children. It describes inner ear abnormalities like Sheibes dysplasia which affects the cochlea and vestibule. It also discusses different types of hearing loss such as conductive, sensory neuronal, and syndromic hearing loss which occurs with other medical problems. The severity of hearing loss is classified from mild to profound based on loudness thresholds. Potential causes include genetic factors, infections during pregnancy, complications at birth, trauma, and certain drugs. Tests used to evaluate hearing include electrocochleography, acoustic reflex testing, tympanometry and audiometry. Management options involve hearing aids, cochlear implants, and developing speech and language skills.























































































