

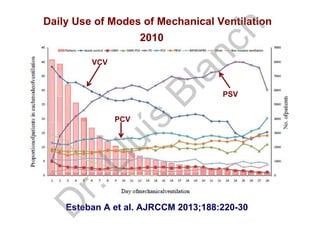

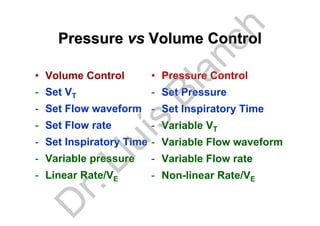



Dr. Lluís Blanch discusses innovations in mechanical ventilation focusing on safety, efficacy, and patient comfort. He highlights various mechanical ventilation modes, protective ventilation strategies, and the effects of neuromuscular blockers on patient outcomes. Additionally, the document examines patient-ventilator interactions, asynchrony, and the importance of managing tidal volume and PEEP in critical care settings.




































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








