This module provides an overview of mechanical ventilation including:
- Common indications for mechanical ventilation including respiratory failure, oxygenation failure, and airway protection.
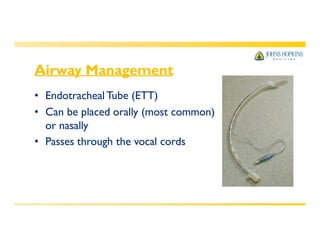
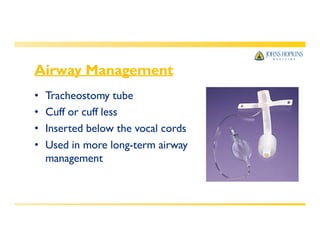
- Types of airways used including endotracheal tubes and tracheostomy tubes.
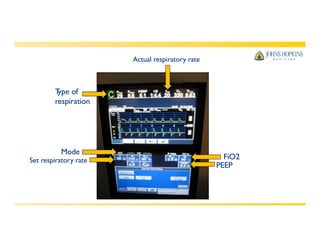
- Common ventilator settings and modes of ventilation such as controlled, assist-control, SIMV, pressure support, and CPAP.
- Potential complications of mechanical ventilation like ventilator dysynchrony, barotrauma, and infections.
- Parameters for assessing patient readiness for weaning such as oxygenation, ventilation, respiratory mechanics, and hemodynamic stability.
![Why is mechanical ventilation
required?
• Impending or existing respiratory failure
• Failure to oxygenate (inadequate exchange of gases at the alveolar
level, as seen in acute respiratory distress syndrome [ARDS])
• Failure to ventilate (decreased mental status or decreased lung
compliance)
• Combination of both
• Airway protection
Cheung AM et al. Am J Respir Crit Care Med. Sep 1 2006;174(5):538-
544. Fletcher SN et al. Crit Care Med. Apr 2003;31(4):1012-1016.
Herridge MS et al. N Engl J Med. Feb 20 2003;348(8):683-693.](https://image.slidesharecdn.com/4-understanding-mechanical-ventilation-220801134916-5675fb8d/85/4-Understanding-Mechanical-Ventilation-pdf-3-320.jpg)