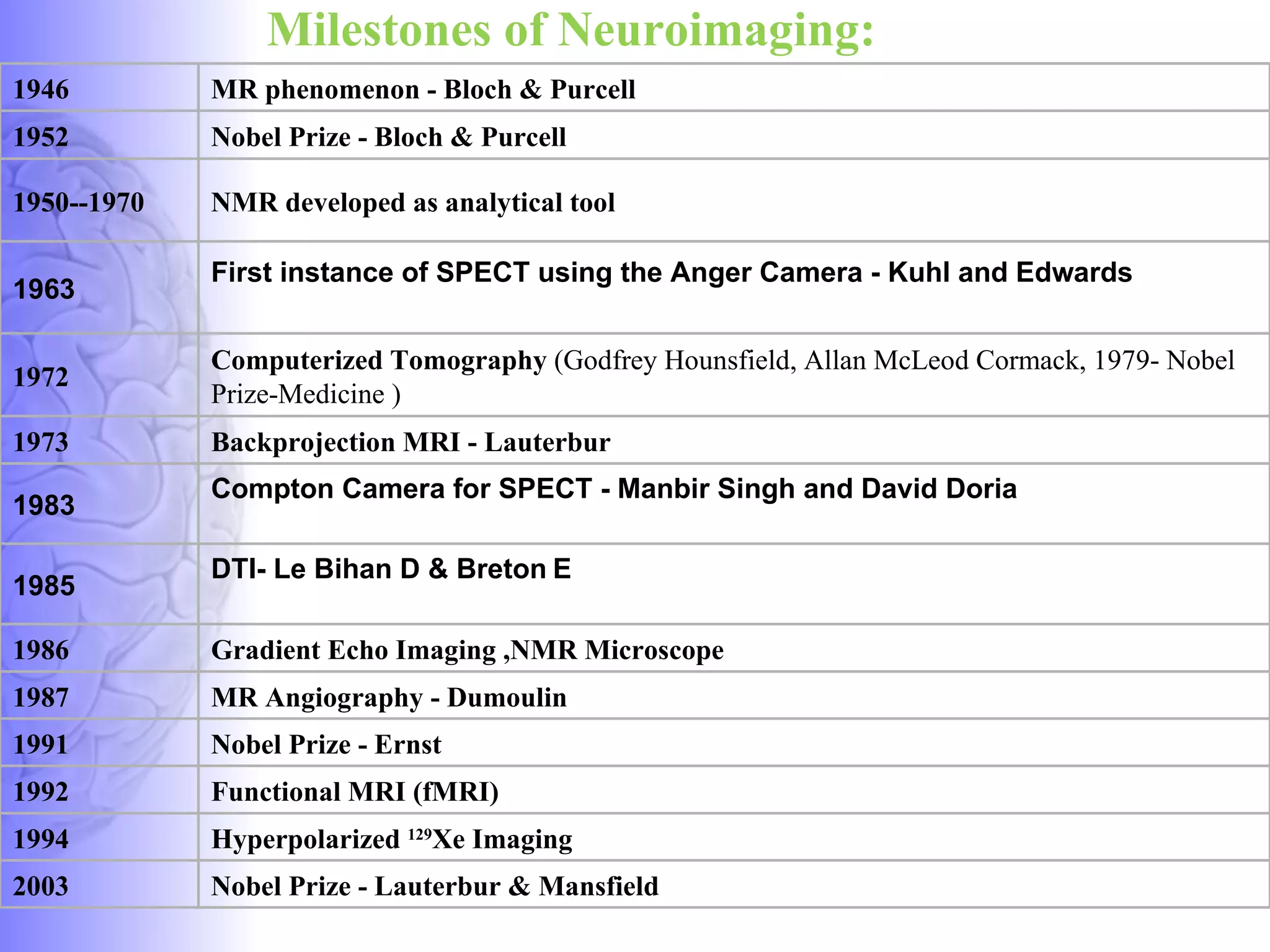
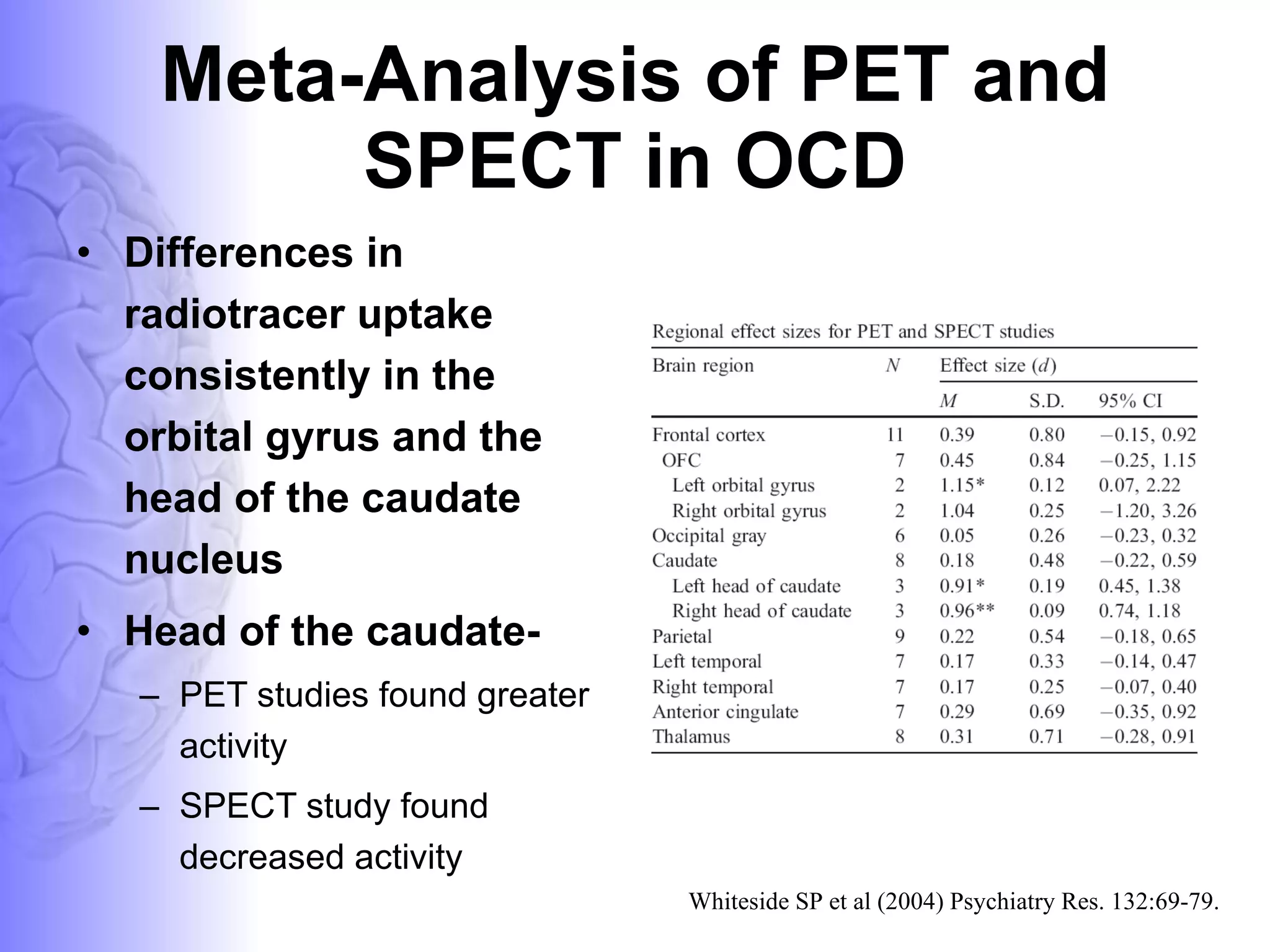
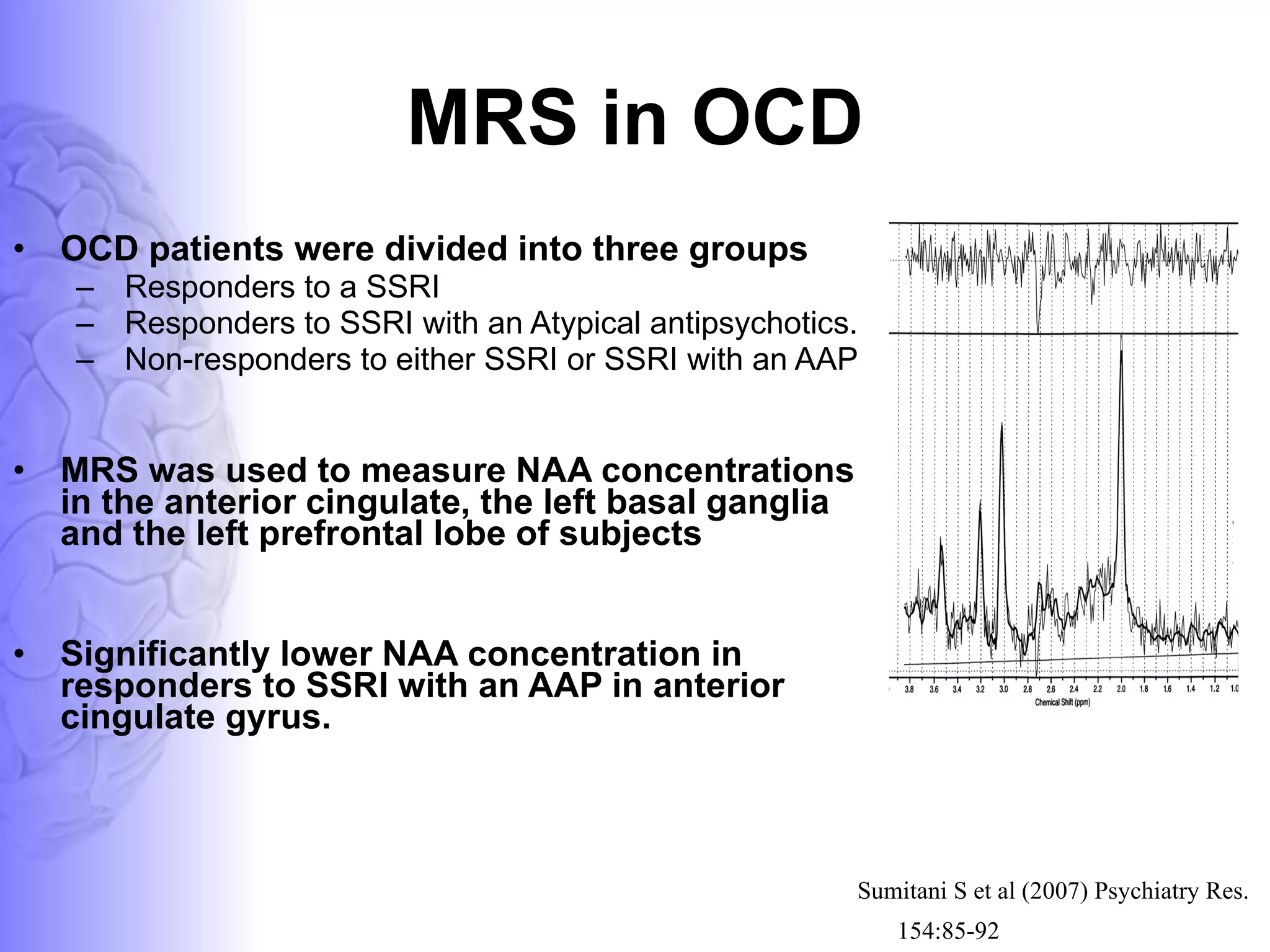
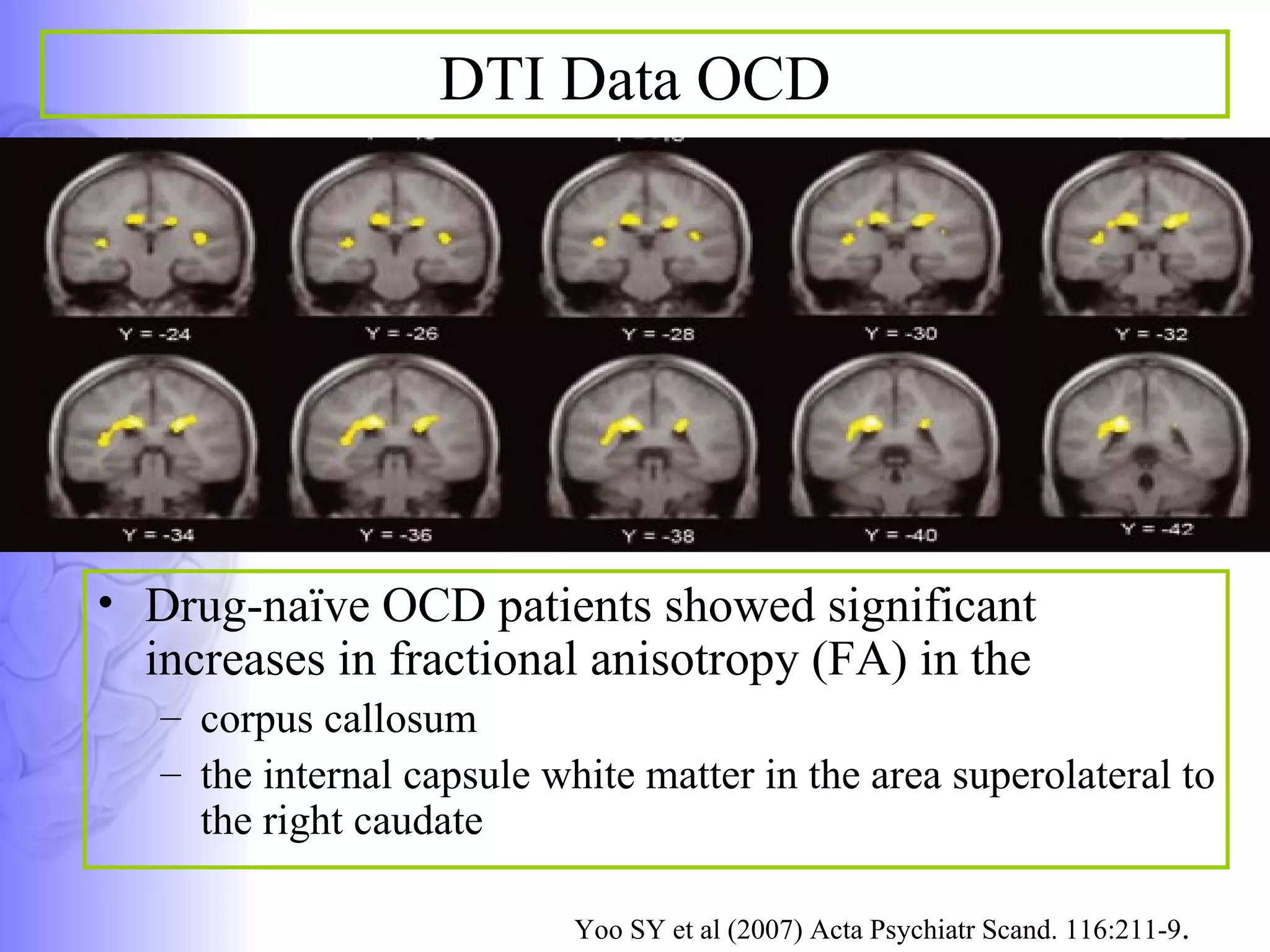



The document provides an overview of neuroimaging techniques used in psychiatry such as MRI, CT, PET, SPECT, fMRI, DTI, and MRS. It discusses the basic principles, milestones in development, and applications of these techniques. Specifically, it summarizes research using these neuroimaging methods that have found abnormalities in brain structure and function in patients with obsessive-compulsive disorder (OCD), such as reduced serotonin transporter binding in fronto-striatal circuits and differences in brain activity in regions like the thalamus and orbitofrontal cortex.



















































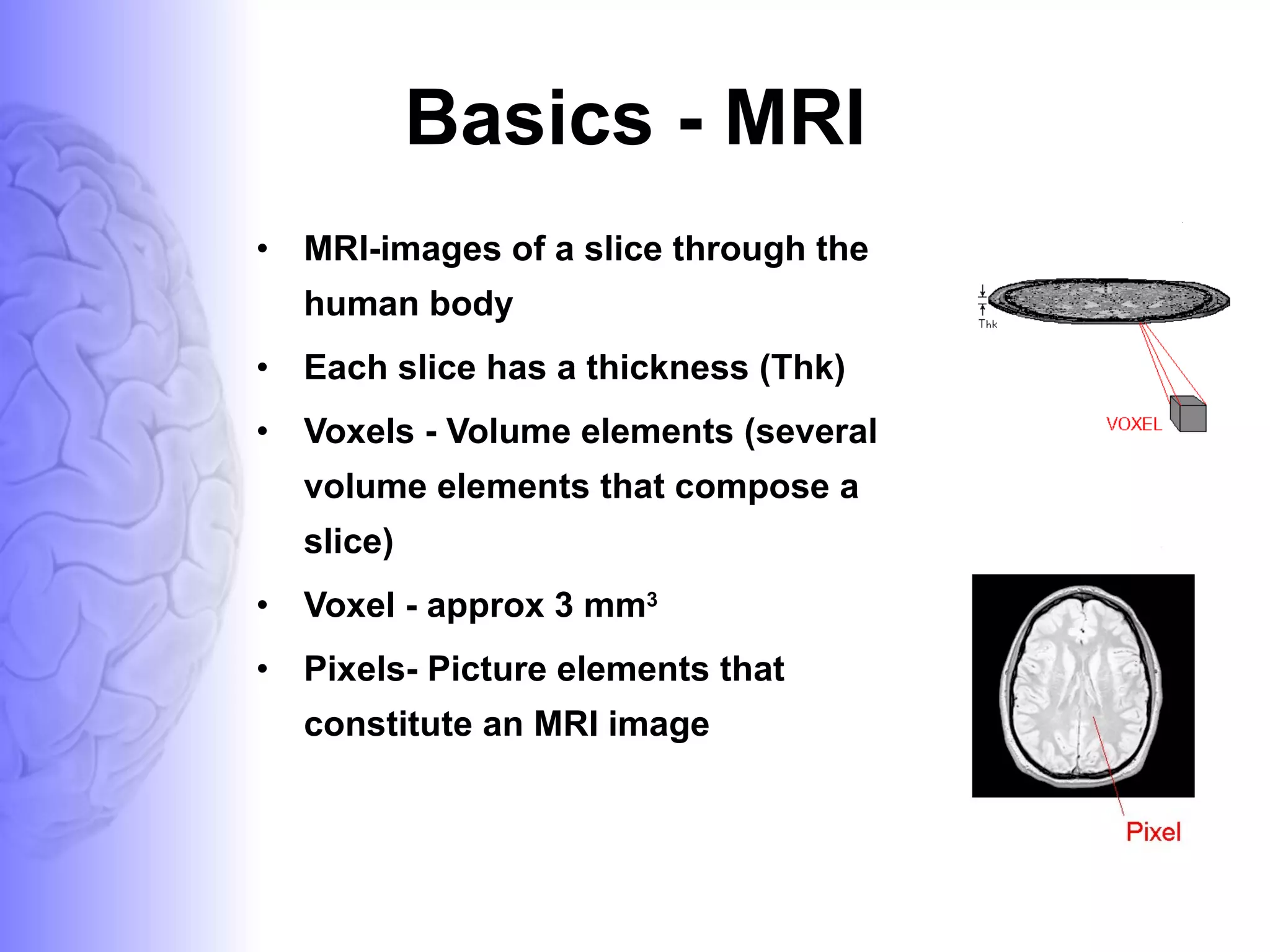
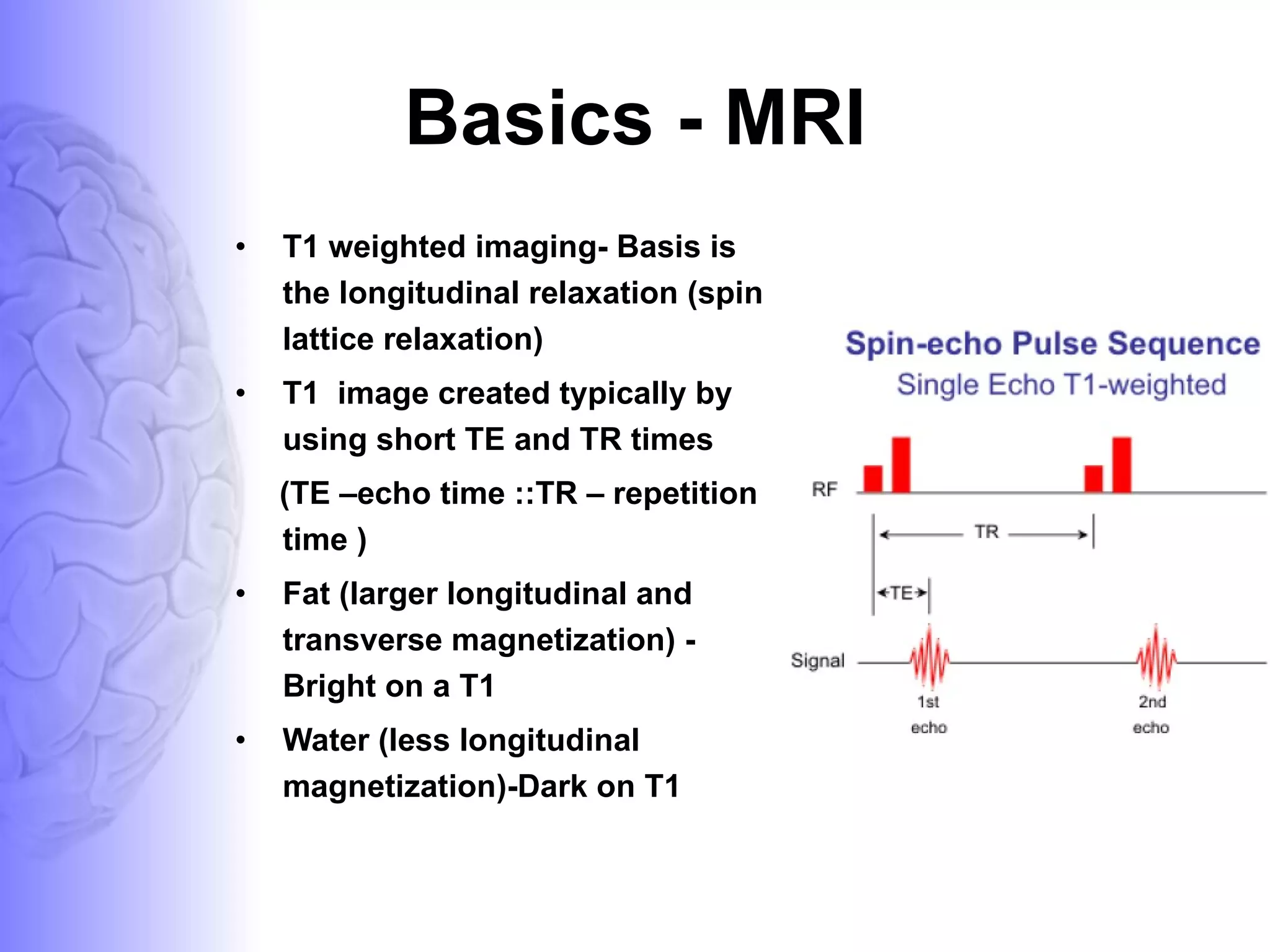
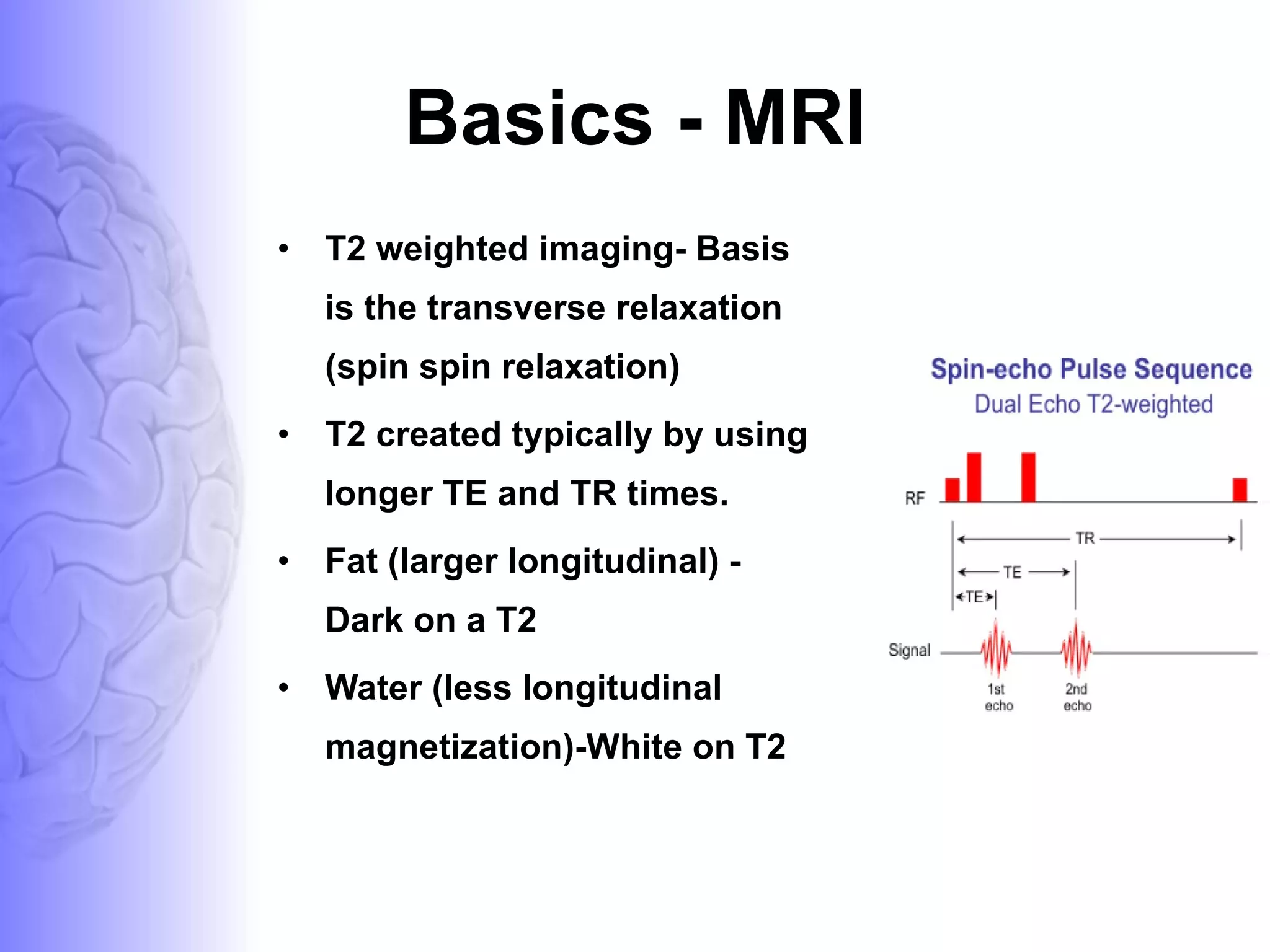
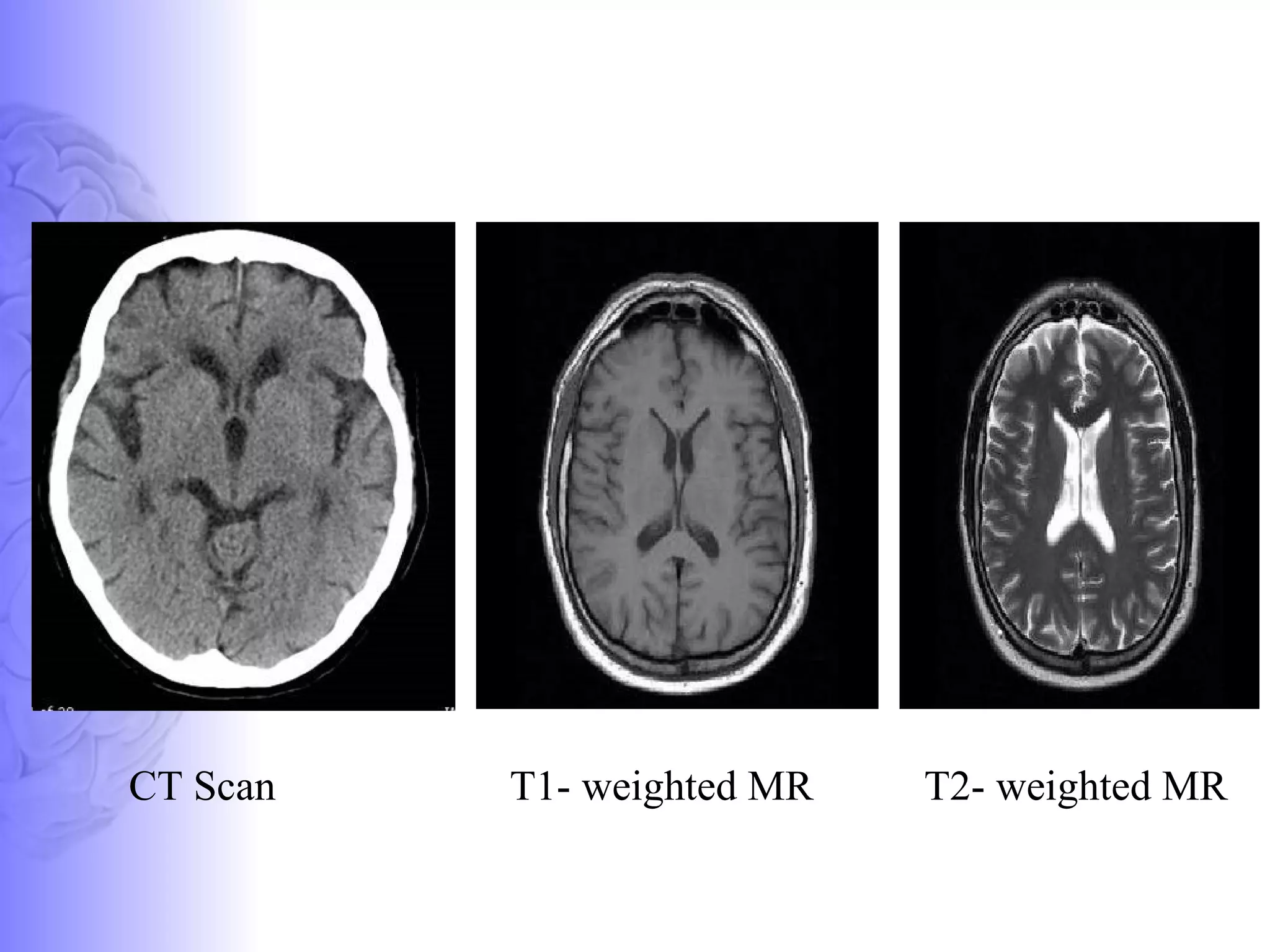
![MAGNETIC_RESONANCE.._IMAGING[MRI][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/magneticresonanceimagingmri1-240903182728-4f857936-thumbnail.jpg?width=640&height=640&fit=bounds)



















![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)
















