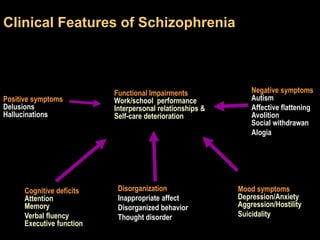
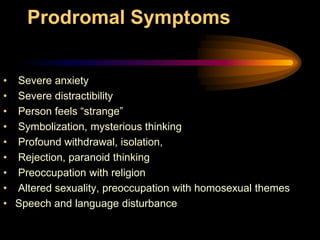





This document provides an overview of the phenomenology of schizophrenia, including a historical perspective on how it has been conceptualized over time. It describes the clinical manifestations and thought disorders commonly seen in schizophrenia, such as formal thought disorders involving disorganized thinking, disorders of thought flow/tempo, disorders of thought possession, and disorders involving delusional thinking. It also briefly discusses misidentification syndromes that can occur.




















![Neuropsychiatry [2017]](https://cdn.slidesharecdn.com/ss_thumbnails/neuropsychiatricmanifestationofcommonneurologicaldisorders-171001003940-thumbnail.jpg?width=640&height=640&fit=bounds)



























































