Downloaded 48 times






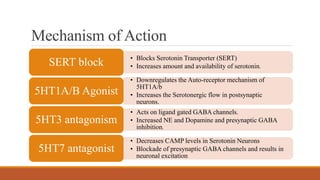












Vortioxetine is a novel antidepressant approved by the FDA in 2013 for the treatment of major depressive disorder. It is manufactured by Takeda Pharmaceuticals and works as a serotonin modulator. It has multiple mechanisms of action including inhibiting the serotonin transporter, acting as an agonist on 5HT1A/B receptors, antagonizing 5HT3 and 5HT7 receptors. Clinical studies showed it was effective in reducing depressive symptoms and had a lower risk of side effects like insomnia compared to SSRIs and SNRIs. Common side effects included nausea, diarrhea and sexual dysfunction. It has a favorable safety and tolerability profile. More long term studies are still needed but it shows promise as a treatment for MDD