Downloaded 382 times
![EEG in OCD:
EEG in OCD
EEG abnormalities present in varying frequency]
Widespread increase in slow waves reported
EEG in Panic
disorders
•25-30% of panic attack patients have
EEG abnormalities
•Helps in differentiating panic attack from
epilepsy
•focal paroxysms of sharp wave activity
coinciding with spontaneous onset of
panic attack is noted](https://image.slidesharecdn.com/12postopdeeg-140113140532-phpapp02/85/eeg-basics-in-psychiatry-22-320.jpg)


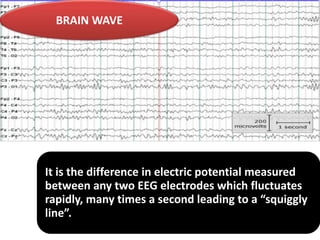
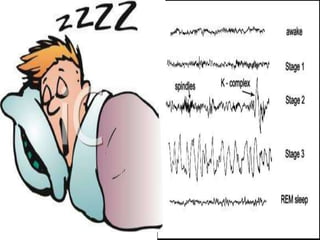
EEG is a non-invasive method to measure electrical activity in the brain. It can help in psychiatry by ruling out physical causes for psychiatric symptoms, aiding in differential diagnosis and treatment selection, and predicting prognosis. EEG findings can provide clues to underlying conditions in disorders like schizophrenia, mood disorders, OCD, panic attacks, dementia, delirium, and substance abuse. However, EEG findings in psychiatry are often nonspecific and EEG has limitations due to only recording cortical activity from the scalp. It currently has no definitive role in diagnosing Axis I or II psychiatric disorders.































































































