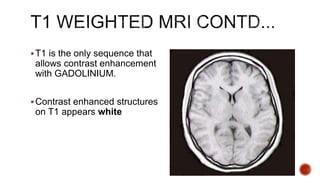
Downloaded 160 times


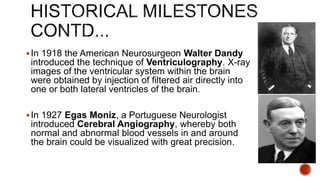
![1946 – MR phenomenon explained by Bloch & Purcell
[1952 – Nobel prize]
1950 – 1970 – NMR developed as an analytical tool
1963 – 1st instance of SPECT using Anger Camera – Kuhn & Edwards
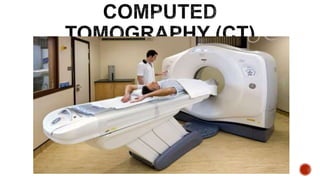
1972 – Computerized Tomography [Godfrey Hounsfield, Alan Mcleod
Cormack,1979 – Nobel prize]
1973 – Backprojection MRI – Lauterbur
1983 – Compton Camera for SPECT – Manbir Singh & David Doria
1985 – DTI – Le Bihan D & Breton E
1986 – Gradient Echo Imaging, NMR Microscope
1987 – MR Angiography – Dumoulin
1992 – Functional MRI by Richard R Ernst
1994 – Hyperpolarized 129 Xe imaging](https://image.slidesharecdn.com/brainimaginginpsychiatry-171129181939/85/Brain-imaging-in-psychiatry-7-320.jpg)
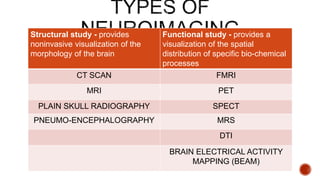
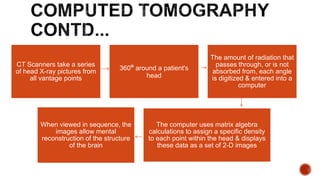


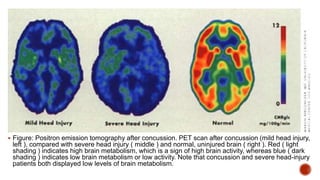

The document discusses the evolution and principles of neuroimaging techniques, including MRI, CT, PET, and SPECT, and their applications in diagnosing psychiatric disorders. It highlights historical milestones in neuroimaging, the methodology behind various imaging techniques, their effectiveness in identifying brain abnormalities, and their roles in patient diagnostics. Key findings suggest that while MRI is preferable for soft tissue differentiation, CT remains essential for acute trauma evaluation, and functional neuroimaging aids in the diagnosis of conditions like dementia.













































![MAGNETIC_RESONANCE.._IMAGING[MRI][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/magneticresonanceimagingmri1-240903182728-4f857936-thumbnail.jpg?width=640&height=640&fit=bounds)




























