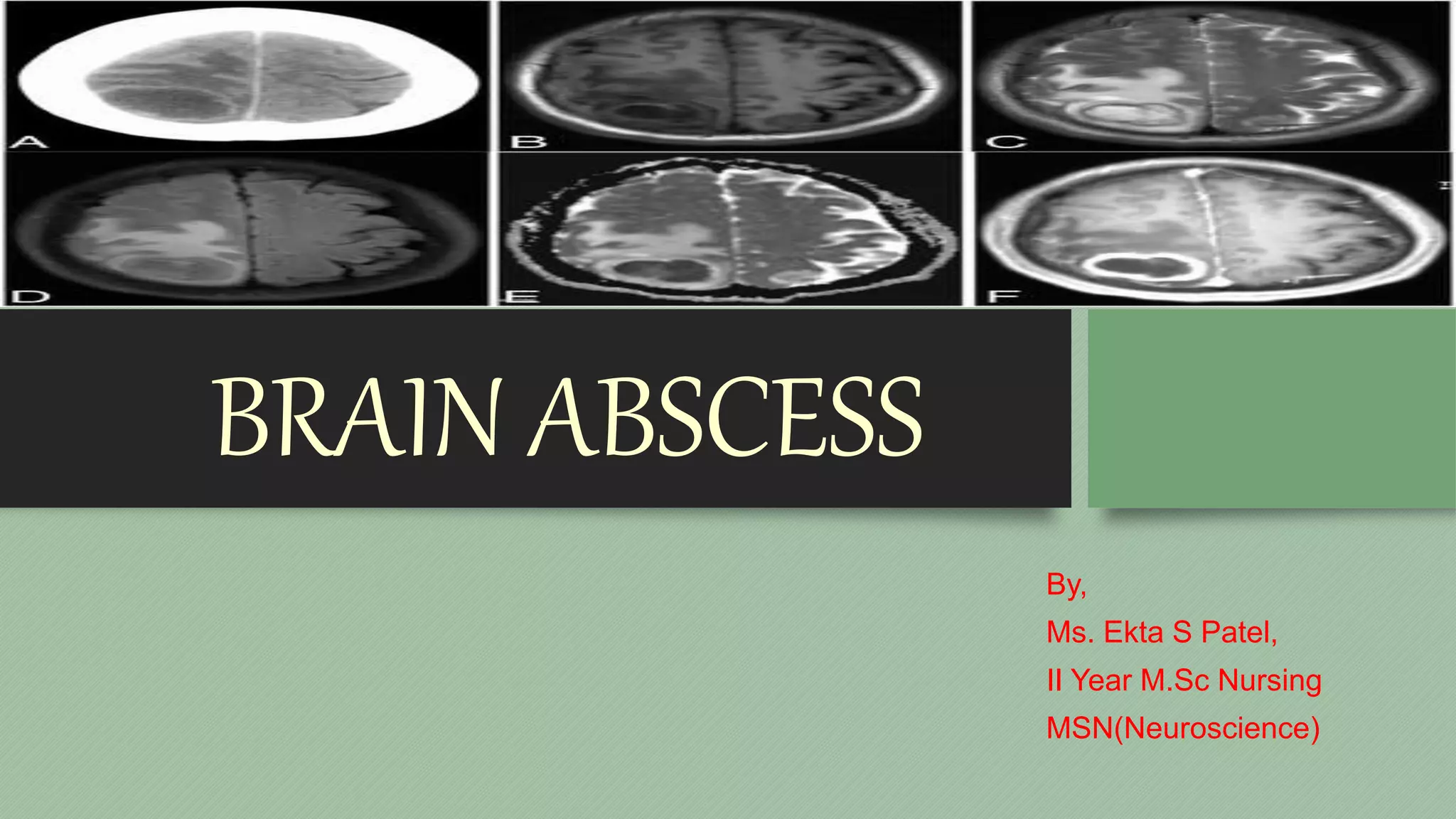
Brain abscess is a collection of pus within the brain tissue caused by a bacterial or fungal infection that can arise from local or distant infectious sources. Symptoms may include changes in mental status, decreased movement and sensation, fever and headache. Diagnosis involves imaging tests and biopsy. Treatment requires antibiotics, sometimes in combination with surgery to drain the abscess, with goals of reducing pressure and swelling in the brain. Even with treatment, brain abscess carries risks of brain damage, recurrence of infection, and long-term neurological deficits.