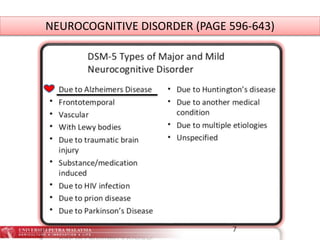
1. Neurocognitive disorders (NCD) encompass disorders where the primary deficit is in cognitive functioning, and are acquired rather than developmental. NCDs can be caused by factors like age, stroke, head injuries, HIV, substance abuse, and neurodegenerative diseases like Alzheimer's and Parkinson's.
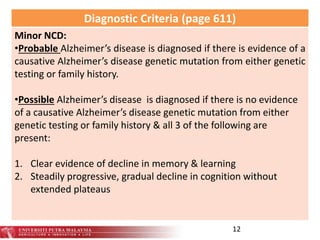
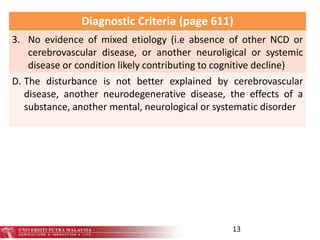
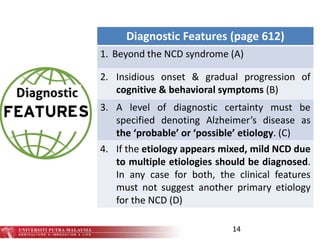
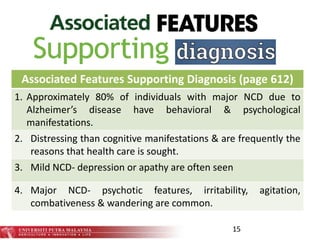
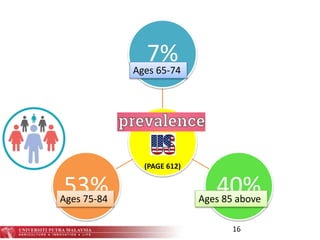
2. For major or mild NCD due to Alzheimer's disease, there must be evidence of decline in memory and learning, as well as impairment in at least two cognitive domains. Features include insidious onset and gradual progression. Risk factors include age, genetic factors, and traumatic brain injuries.
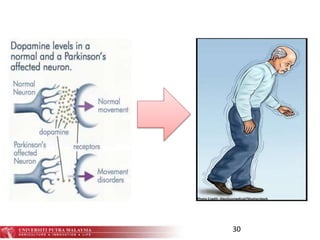
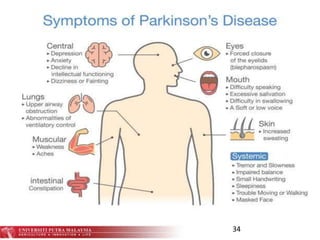
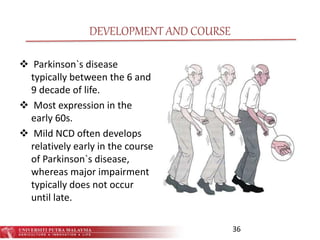
3. Parkinson's disease is a neurocognitive disorder involving degeneration of motor control centers in the brain























![Neurocognitive Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ncd2020v2-200526001756-thumbnail.jpg?width=640&height=640&fit=bounds)
































































