Download as PDF, PPTX



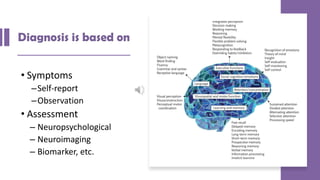



![Mix all ingredients except the
oil for about 2 min or until smooth
Have all the
ingredients
Make three long, thick dough strips and then make them
like a doughnut shape and connect the 2 sides really well
Put the oil in a medium sized pan
on the stove set on med or med high
Keep in for approximately
7 minutes or until gold
Let cool and enjoy!
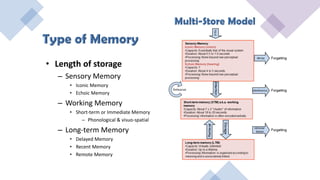
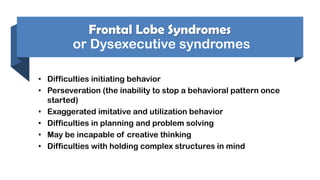
Sequence operations or events to accomplish a goal
When warm gently
Place in one doughnut
Sequencing [Planning]
How To Make A Doughnut](https://image.slidesharecdn.com/ncd2020v2-200526001756/85/Neurocognitive-Disorders-2020-27-320.jpg)
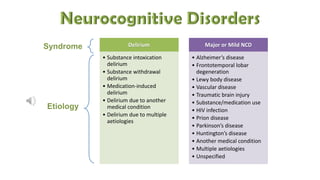
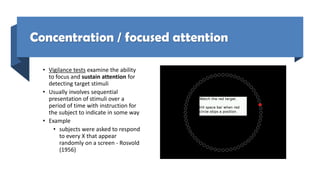
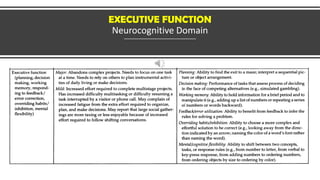
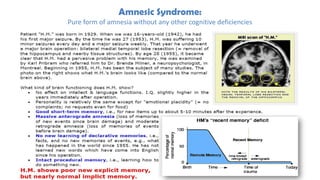
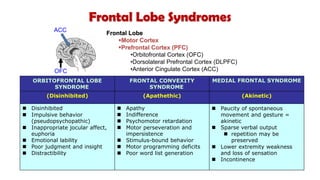
![Tower of Hanoi
Frontal Lobe Test
Task: Move all 3 disc to peg 3
Rule: 1) move one disc at a time
2) larger disc cannot be placed on smaller one
3) subjects must solve problem “in their head”
Executive processes involved
1. [selective attention] executive attention
2. [mental flexibility] switching attention
3. Updating working memory
4. Setting a goal and analysis of sub-goals
5. Sequencing of steps
Frontal-lobe patients, particularly patients with damage to the DLPFC,
perform poorly on the Tower of Hanoi problem (Shallice, 1982)](https://image.slidesharecdn.com/ncd2020v2-200526001756/85/Neurocognitive-Disorders-2020-28-320.jpg)
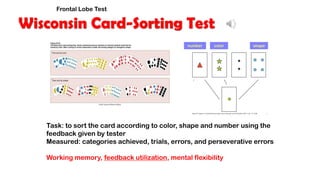
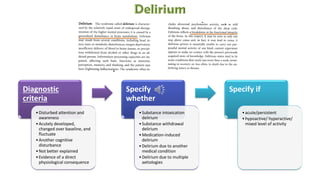
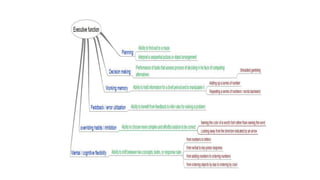
![Motor Cortex
Superior
Temporal Cortex
Occipital Cortex
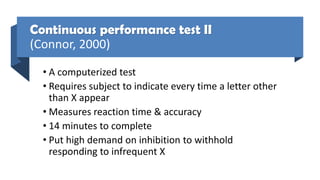
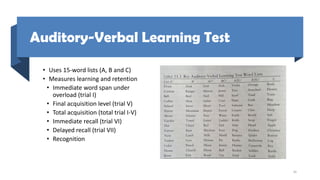
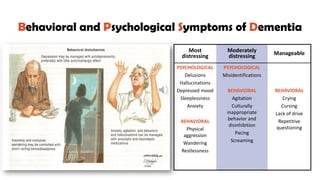
Overriding Habits
STROOP TEST
State the color as fast as you can
color
GREEN
word
RED
RED
GREEN
Conflict
Monitor
[cingulate]
Attention
Controller
[DLPFC]
INPUT RESPONSE
DLPFC=dorsolateral prefrontal cortex](https://image.slidesharecdn.com/ncd2020v2-200526001756/85/Neurocognitive-Disorders-2020-37-320.jpg)
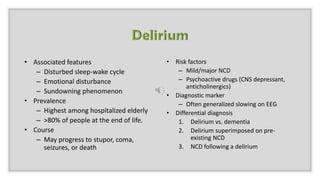
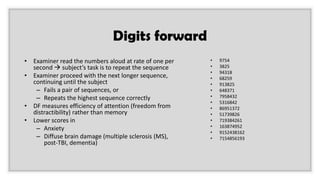
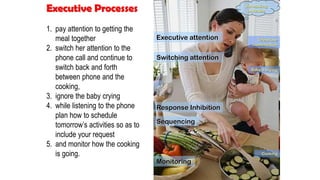
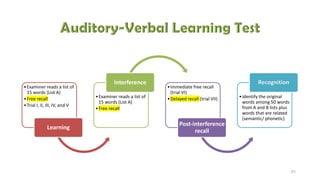
![PRESS
PRESS
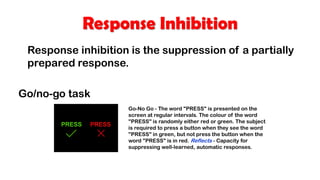
Go trials, when no inhibition is required
Dorsolateral prefrontal [DLPFC] cortex is activated
No-go trials, when response inhibition is required
DLPFC + Orbitofrontal cortex is activated
1) orbitofrontal cortex
2) lateral prefrontal cortex
3) ventromedial cortex
4) limbic system
Response Inhibition](https://image.slidesharecdn.com/ncd2020v2-200526001756/85/Neurocognitive-Disorders-2020-40-320.jpg)

![Social Cognition [comportment]
"Comportment" is a term that refers to social behavior, insight, and
"appropriateness" in different social contexts. Normal comportment
involves having insight and the ability to recognize what behavior is
appropriate in a particular social situation and to adapt one's behavior
to the situation.
For example, while it may be perfectly natural and acceptable to take
one's shoes and socks off at home, it is probably not the thing to do
while in a restaurant.](https://image.slidesharecdn.com/ncd2020v2-200526001756/85/Neurocognitive-Disorders-2020-59-320.jpg)

![Behavior in Dementia
Behavior is often disorganized, inappropriate, distractible, and restless.
There are a few sign of initiative. Changes in personality may manifest as
an antisocial behavior, which sometimes include sexual disinhibition or
shoplifting.
Goldstein (1975) describes the ways in which behavior can be affected by
cognitive defects. Typically there is reduction of interests [shrinkage of
milieu] and, rigid and stereotyped routines [organic orderliness] and,
when the person is taxed beyond restricted abilities, a sudden explosion
of anger or other emotion [catastrophic reaction]](https://image.slidesharecdn.com/ncd2020v2-200526001756/85/Neurocognitive-Disorders-2020-64-320.jpg)
![Frontotemporal Dementia
FTD is associated with Kluver-Bucy syndrome [KBS]. The most common
symptoms of KBS in FTD is hyperorality manifested as bingeing, altered food
preferences especially for sweets, food fads, weight gain or increased smoking](https://image.slidesharecdn.com/ncd2020v2-200526001756/85/Neurocognitive-Disorders-2020-65-320.jpg)

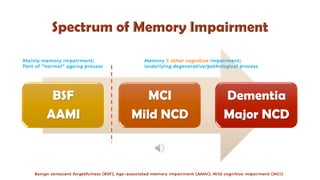
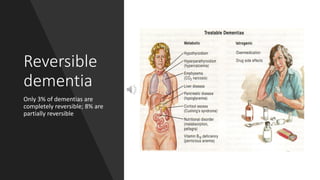
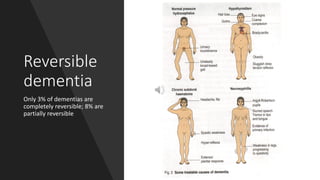
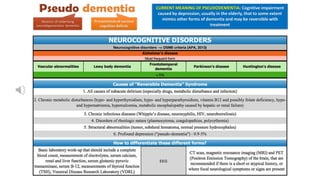
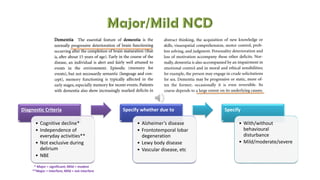
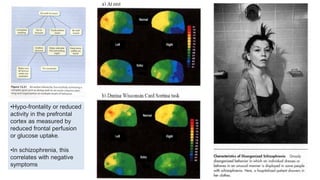
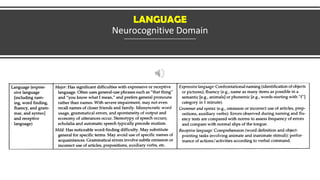
Mild cognitive impairment (MCI) and dementia exist on a continuum, with MCI representing a stage between expected cognitive decline of normal aging and more serious decline associated with dementia. MCI is characterized by memory impairment greater than normal aging but not significantly interfering with daily life, while dementia involves memory and other cognitive impairments that do interfere with daily functioning. Only a small percentage of dementias are potentially reversible through treatment of underlying causes.






















































![Kesejahteraan Emosi di Tempat Kerja [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/kesejahteraanemosi2020-200905072541-thumbnail.jpg?width=640&height=640&fit=bounds)
![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)



![Non-delusional Morbid Jealousy [2019]](https://cdn.slidesharecdn.com/ss_thumbnails/56201795113132228753-190801100249-thumbnail.jpg?width=640&height=640&fit=bounds)



























