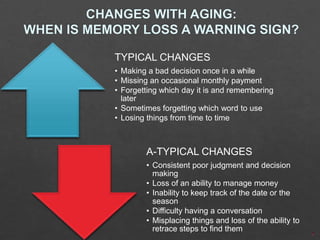
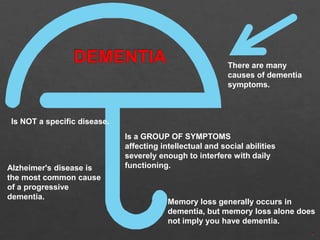
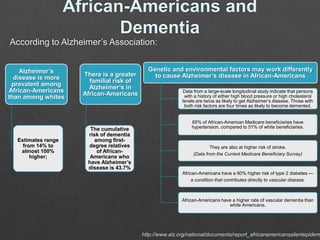
The document outlines a presentation on various types of dementia, emphasizing atypical changes in behavior and cognition that differentiate Alzheimer's from other dementias. It highlights the increased risk of Alzheimer's disease among African Americans, citing genetic, environmental, and health factors. Additionally, the document discusses treatment options, prevalence rates, and the role of the Alzheimer's Association in supporting research and care for affected individuals.