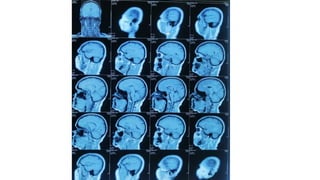
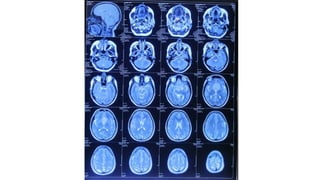
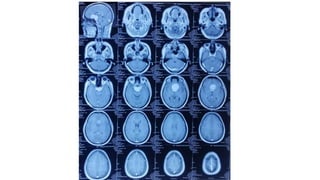
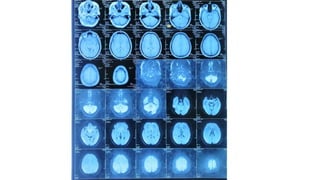
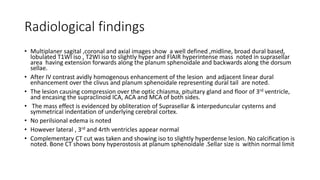
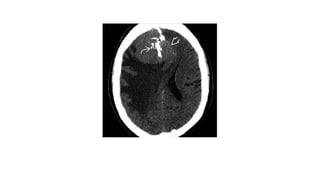
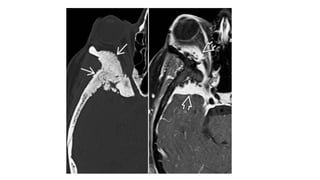
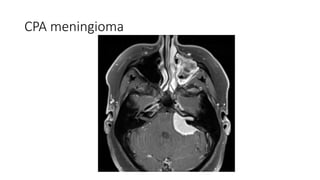
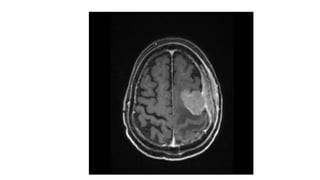
A 40-year-old female presented with progressive vision impairment and headaches. MRI showed a well-defined suprasellar mass compressing surrounding structures and enhancing with a dural tail. Radiological findings were consistent with a suprasellar meningioma extending along the planum sphenoidale and dorsum sellae. Meningiomas typically originate from arachnoid cells, are most common in the supratentorial compartment, and demonstrate avid enhancement with a dural tail on MRI. Surgical resection aims to remove the tumor and involved dura.



















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















