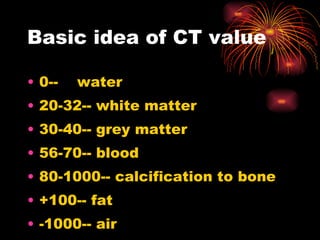
This document provides an overview of various medical imaging modalities used to image intracranial lesions, including their uses and basic interpretations. It discusses simple radiography, CT, MRI, ultrasound, angiography, nuclear medicine scans, and PET. It also outlines the basics of reading and interpreting a CT brain scan, such as identifying anatomical structures and analyzing lesions to make diagnoses or differential diagnoses.