Downloaded 20 times




















![MEDIAN NERVE
• Formation: from two roots from lateral cord [C(5),6,7]& from medial
cord(C8,T1) of brachial plexus
• • These two roots embrace the third part of axillary artery uniting
anterior or lateral to it](https://image.slidesharecdn.com/nervesofhand-210610175234/75/Nerves-of-hand-33-2048.jpg)











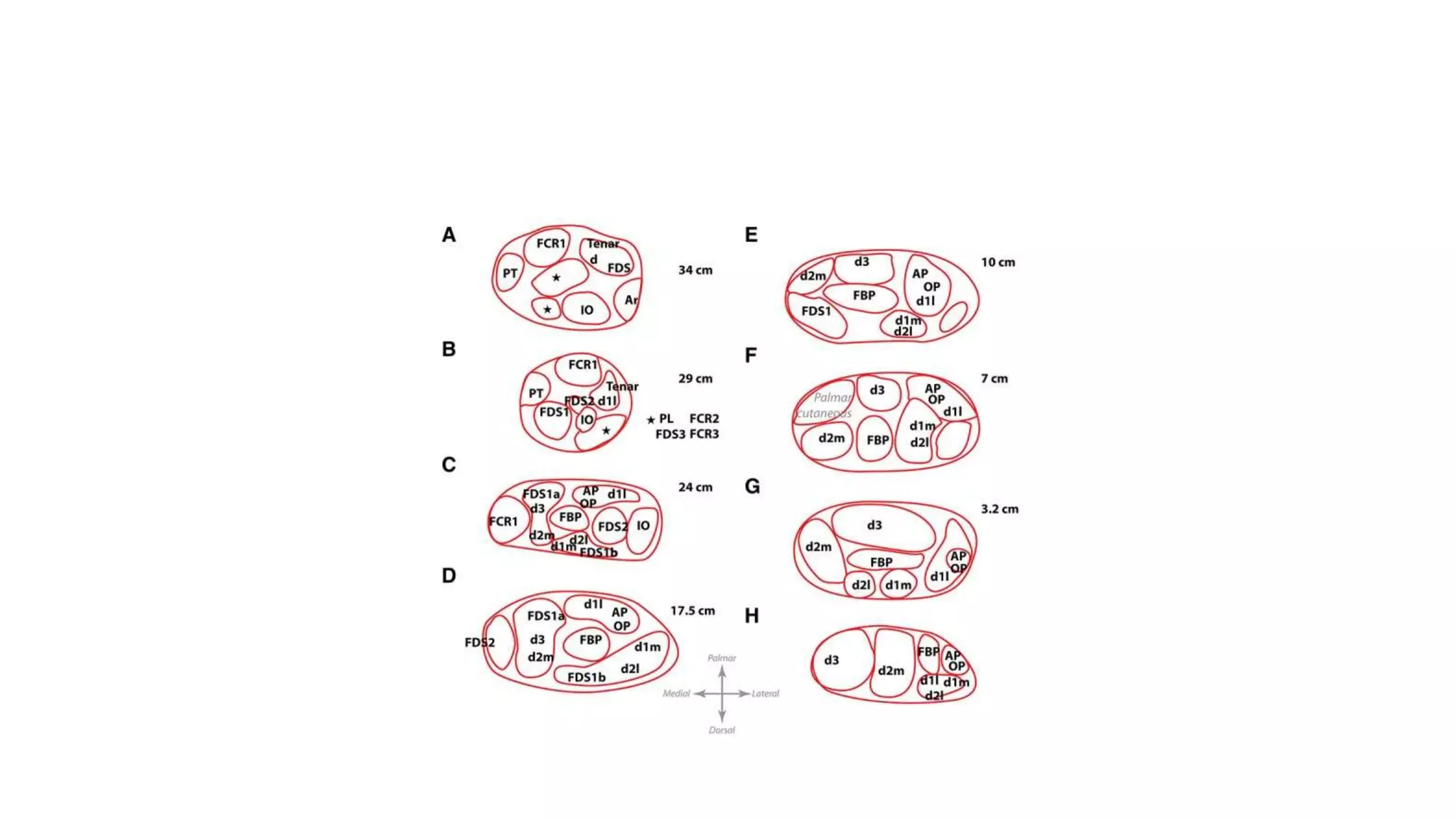
![Pattern of topographic distribution of median nerve motor fascicles. The median nerve was sectioned in 2
palmar (radial and ulnar) and 2 dorsal (radial and ulnar)
quadrants each, according to black lines in the oval. The motor fascicles were assigned to the quadrants. The
size of the squares represents the frequency of the observed
fascicles’ locations and their ratios are given [%]. d, dorsal; n, sample size; p, palmar; r, radial; u, ulnar](https://image.slidesharecdn.com/nervesofhand-210610175234/75/Nerves-of-hand-49-2048.jpg)
![Pattern of topographic distribution of
median nerve sensory fascicles. The median
nerve was sectioned in 2 palmar (radial and
ulnar) and 2 dorsal (radial and ulnar)
quadrants each, according to black lines in
the oval. The sensory fascicles were
assigned to the quadrants. The size of the
squares represents the frequency of the
observed
fascicles’ locations and their ratios are given
[%]. The numeric values are rounded to one
decimal with the result that the numeric
values partially vary from 100. (a) Palmar
cutaneous branch (PCB) and thumb, (b)
index finger, (c) middle finger, (d) ring finger
and communicating branch of median nerve
with ulnar nerve. d, dorsal; n, sample size;
p, palmar; r, radial; u, ulnar; asterisk, the
missing sample was supplied by the ulnar
nerve](https://image.slidesharecdn.com/nervesofhand-210610175234/75/Nerves-of-hand-50-2048.jpg)



The document summarizes the anatomy and branches of the ulnar, radial, and median nerves in the upper limb. It describes the course and branches of each nerve in the axilla, arm, and forearm. It also discusses the separation of motor and sensory components within the nerves and provides diagrams of fascicular patterns. Key points include that the ulnar nerve supplies medial forearm muscles and skin of the little and half of the ring finger, the radial nerve innervates posterior forearm muscles and skin of the dorsal hand, and the median nerve gives branches in the forearm and palm.























































































