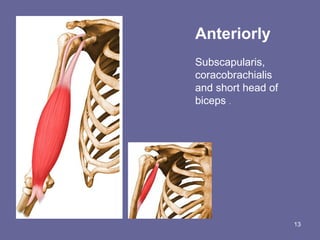
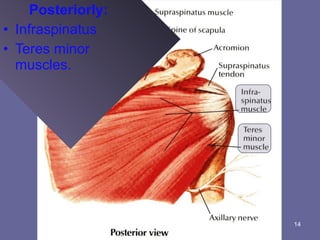
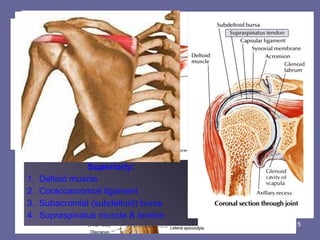
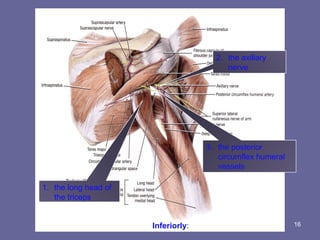
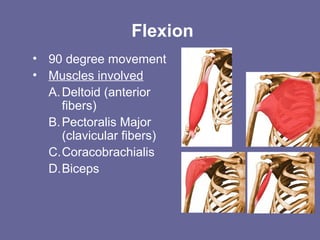
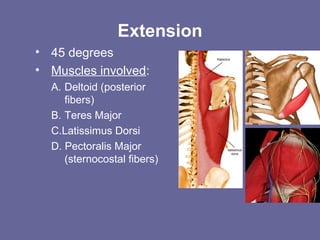
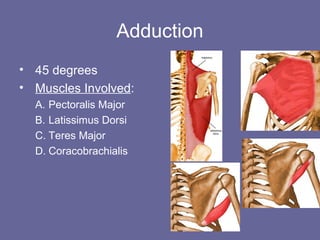
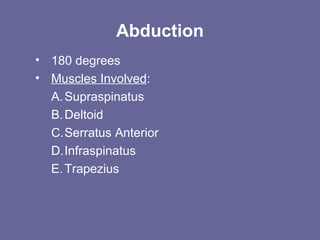
The shoulder joint is comprised of three bones and three joints: the scapula, clavicle, and humerus. It allows for flexion, extension, abduction, adduction, external rotation, and internal rotation. Stability is provided by ligaments like the glenohumeral ligament and muscles like the rotator cuff. Common injuries include dislocations, rotator cuff tears, and tendonitis which can cause pain and limited mobility.