Download to read offline





![ Effacing web/release contracture (similar to first listed use)
Closing cutaneous defects (eg, large oval defects, pharyngocutaneous
fistulae)
Correcting stenosis (eg, tracheostoma, nares, external auditory canal) using
single or multiple Z-plasties [3]
Transposing healthy tissue to close a fistula (eg, tracheostoma closure after
irradiation)](https://image.slidesharecdn.com/newmicrosoftpowerpointpresentation-210610175851/85/Suture-techniques-Z-plasty-15-320.jpg)
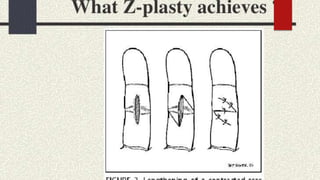
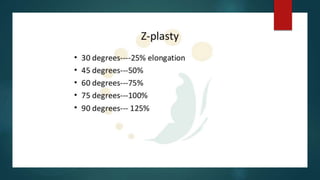

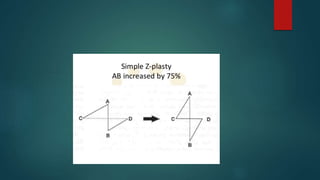
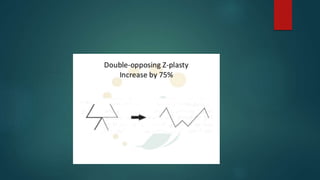
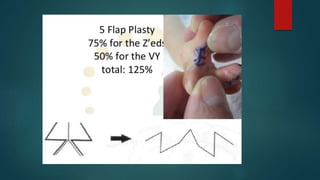


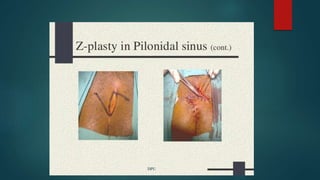



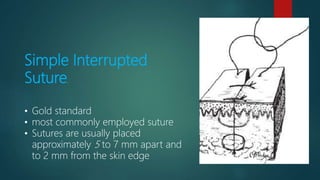
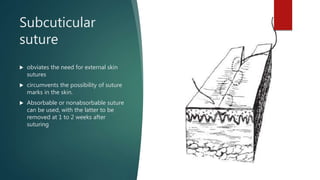
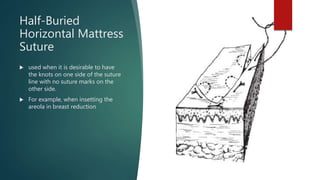
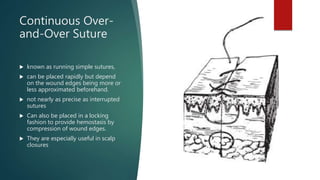
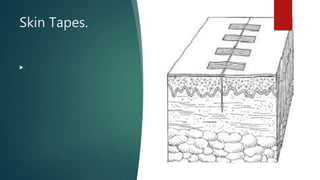
The document describes various suture techniques including simple interrupted sutures, which are the gold standard, subcuticular sutures which avoid external knots, half-buried horizontal mattress sutures which keep knots on one side, continuous over-and-over sutures which can be placed rapidly but are less precise than interrupted sutures, skin staples which are a timesaving alternative to sutures, skin tapes and adhesives which can be used in low tension areas, and Z-plasties which help prevent or limit scarring and contractures. It also outlines indications, contraindications and potential complications of Z-plasty techniques.







































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











