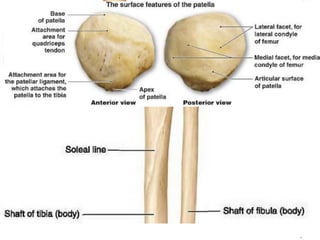
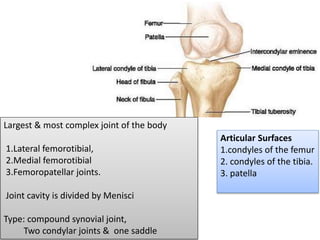
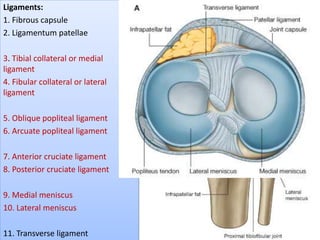

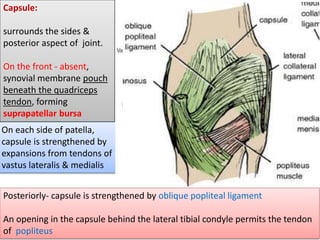







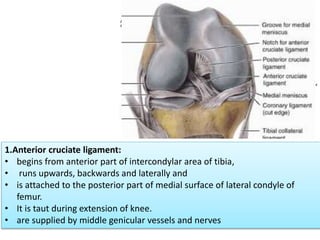



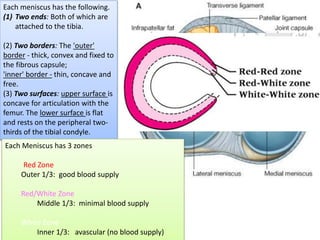
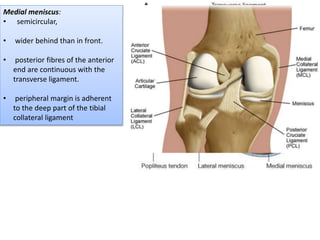


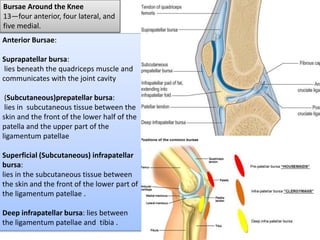



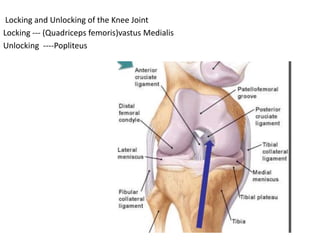




The knee joint is a compound synovial joint composed of the femorotibial joints laterally and medially, and the femoropatellar joint. It contains articular surfaces on the femoral condyles and tibial plateaus, and the patella. The joint cavity is divided by the medial and lateral menisci. Stability is provided by ligaments like the ACL, PCL, MCL and LCL. Muscles like the quadriceps and hamstrings facilitate movement of the knee.























































































