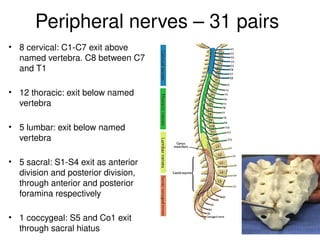
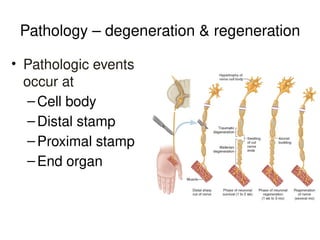
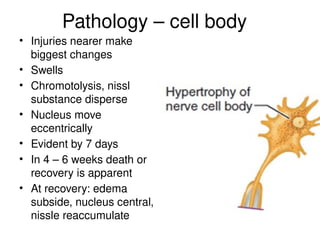
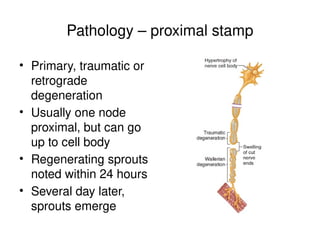
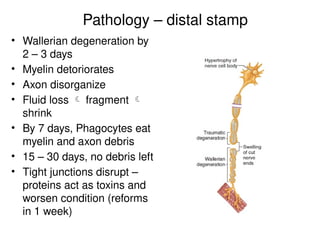
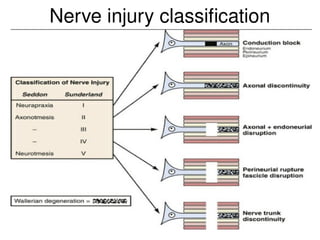
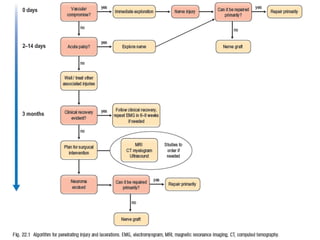
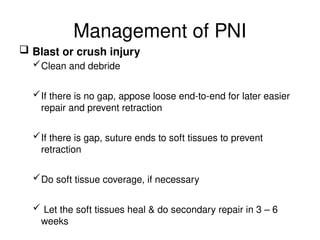
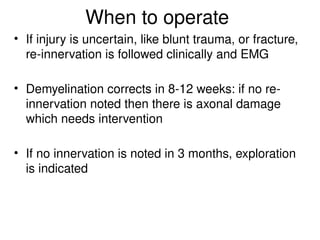
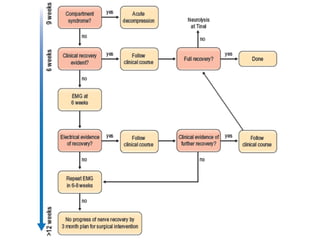
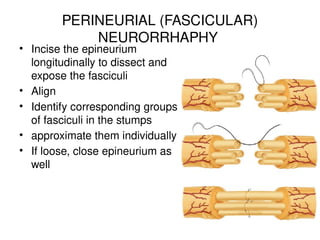
El documento detalla la anatomía, patología, características y tratamiento de las lesiones de nervios periféricos, describiendo la estructura del sistema nervioso y los tipos de lesiones que pueden ocurrir. Se analizan los mecanismos de degeneración y regeneración nerviosa, así como los métodos de diagnóstico y las opciones de tratamiento, incluida la cirugía. Se enfatiza la importancia de la intervención temprana y la alineación adecuada de los fascículos nerviosos para una recuperación efectiva.












































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















