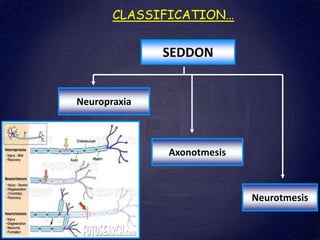
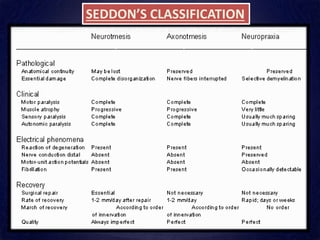
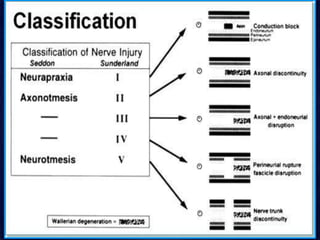
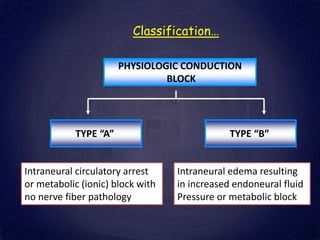
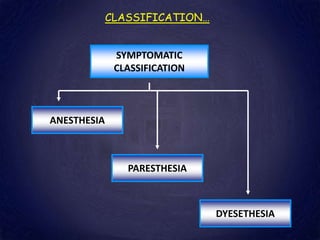
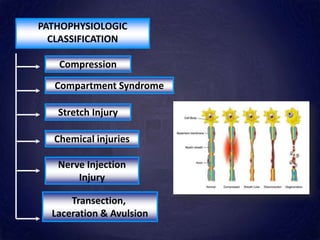
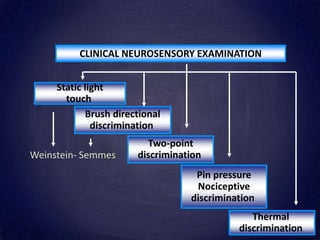
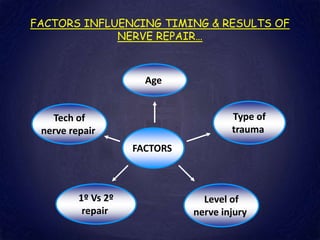
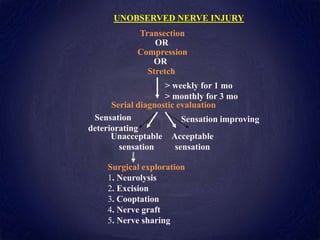
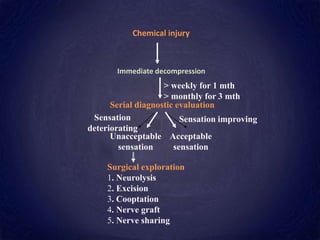
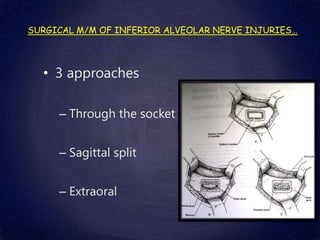
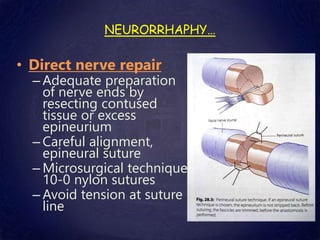
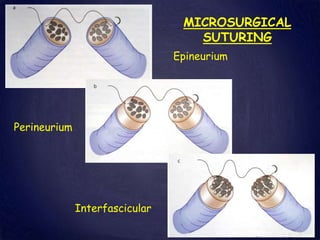
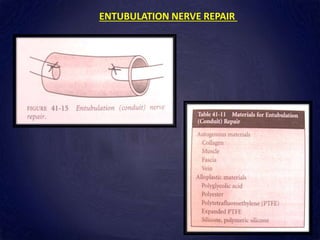
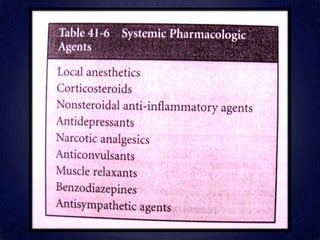
Nerve injuries can occur from trauma, surgery, or other causes. They are classified based on the severity and type of injury. Minor injuries may heal on their own while more severe injuries require surgical repair. The goal of treatment is to promote regeneration of injured nerves. This involves classifying the injury, evaluating it clinically, and managing it through observation, surgery such as neurorrhaphy, or non-surgical means like physical therapy. Proper classification, management, and repair techniques can help improve outcomes from nerve injuries.


















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


